Although the world is becoming mostly sedentary, our bodies still require a wide variety of daily movements in order to work well. Many of us struggle to get regular exercise, but even that can fall short of nourishing the body from head to toe. How can we move more—a lot more—when we have sore, stiff parts and overly busy lifestyles? Join Katy Bowman M.S., biomechanist, author, and movement educator as she combines big-picture lessons on biomechanics, kinesiology, physiology, and natural hu ...
…
continue reading
Content provided by CardioNerds. All podcast content including episodes, graphics, and podcast descriptions are uploaded and provided directly by CardioNerds or their podcast platform partner. If you believe someone is using your copyrighted work without your permission, you can follow the process outlined here https://player.fm/legal.
Similar to Cardionerds: A Cardiology Podcast
Introducing the BODi® Partner Podcast, the official podcast channel devoted exclusively to BODi Partners. From archives of the BODi Wake-Up Call, I Am BODi stories, and What I Know Now success tips from seasoned Partners, this podcast is your one-stop source for personal development, business training and peer-to-peer inspiration. Ready to explode your business? Tune in regularly to our official podcast and join the ranks of those transforming their lives and the lives of others!
…
continue reading
Join expert voices from Barbell Logic and others from the world of strength for resources to help you get strong for life. Get coaching options and more educational content at barbell-logic.com.
…
continue reading
PT Inquest is an online journal club. Hosted by Jason Tuori, Megan Graham, and Chris Juneau, the show looks at an article every week and discusses how it applies to current physical therapy practice.
…
continue reading
We are often distracted in life and never really dive deep into the real foundation of self improvement, goal achieving, and wellbeing. - Join our team of experts every week as we discuss the real facets of manhood. Topics like: How to develop more self esteem, self love, deeper relationships. How to improve our wellbeing, mental toughness, resilience, and productivity. How to develop critical skills, become better leaders, expand our careers/business, create financial security and contribut ...
…
continue reading
The Art of Charm is where self-motivated people, just like you, come to learn from the company’s coaches about to how to master human dynamics, relationships, and becoming your best self with the help of Johnny and AJ, the company’s founders. Johnny and AJ bring their 11 years of coaching experience from their famous Bootcamps, where they host clients in Los Angeles from all over the world and they share their stories, best practices and themselves on this weekly podcast. Not only does The A ...
…
continue reading
Seeking a healthier emotional life? It’s time to bring a trained psychologist and mental health expert along for the ride. Dr. Monica Johnson explains the why behind complex emotions, helps you form better relationships, and guides you down the path of self-understanding.
…
continue reading
For the complete newbie or the experienced hypnotist, Brain Software with Mike Mandel is the world's most interesting, educational and fun podcast discussing hypnosis, NLP and strategies for peak performance and self improvement. Mike Mandel is a 6-time award winning hypnotist, immensely popular keynote speaker, stage performer, psychotherapist and NLP trainer. He has been doing hypnosis since he was 12 years old. Mike has an amazing ability to demystify hypnosis, teach core concepts, and te ...
…
continue reading
Welcome to Almost 30 - a supportive space to fuel your conscious evolution. Join us, LA-based best friends Krista Williams and Lindsey Simcik, for heart-centered, hilarious conversations and real, raw, impactful interviews with brilliant guests. We dive deep into topics like modern spirituality to health and wellness, aliens to entrepreneurship, social justice, and self development. With every episode, our mission is to empower you, expand what you think is possible and, make you laugh - a l ...
…
continue reading
The American healthcare system is one of the most innovative in the world. But it’s also riddled with complex challenges, such as access to affordable medications, inefficiency and administrative burdens, and communication barriers between providers. There’s clearly a better way—and at Surescripts, we have a unique sightline into what that may be. In this series, host Melanie Marcus, Chief Marketing Officer of Surescripts, sits down with today’s most inspiring and innovative leaders in healt ...
…
continue reading
Player FM - Podcast App
Go offline with the Player FM app!
Go offline with the Player FM app!

))
371. Case Report: The Curious Case of Obstructive Cardiogenic Shock – Maine Medical Center
Manage episode 418121214 series 2585945
Content provided by CardioNerds. All podcast content including episodes, graphics, and podcast descriptions are uploaded and provided directly by CardioNerds or their podcast platform partner. If you believe someone is using your copyrighted work without your permission, you can follow the process outlined here https://player.fm/legal.
CardioNerds Dr. Josh Saef and Dr. Tommy Das join Dr. Omkar Betageri, Dr. Andrew Geissler, Dr. Philip Lacombe, and Dr. Cashel O’Brien from the Maine Medical Center in Portland, Maine to enjoy an afternoon by the famous Portland headlight. They discuss a case of a patient who presents with obstructive cardiogenic shock. Dr. Bram Geller and Dr. Jon Donnelly provide the Expert CardioNerd Perspectives & Review segment for this episode. Dr. Maxwell Afari, the Maine Medical Center cardiology fellowship program director highlights the fellowship program. Audio editing by CardioNerds Academy Intern, student doctor Tina Reddy.
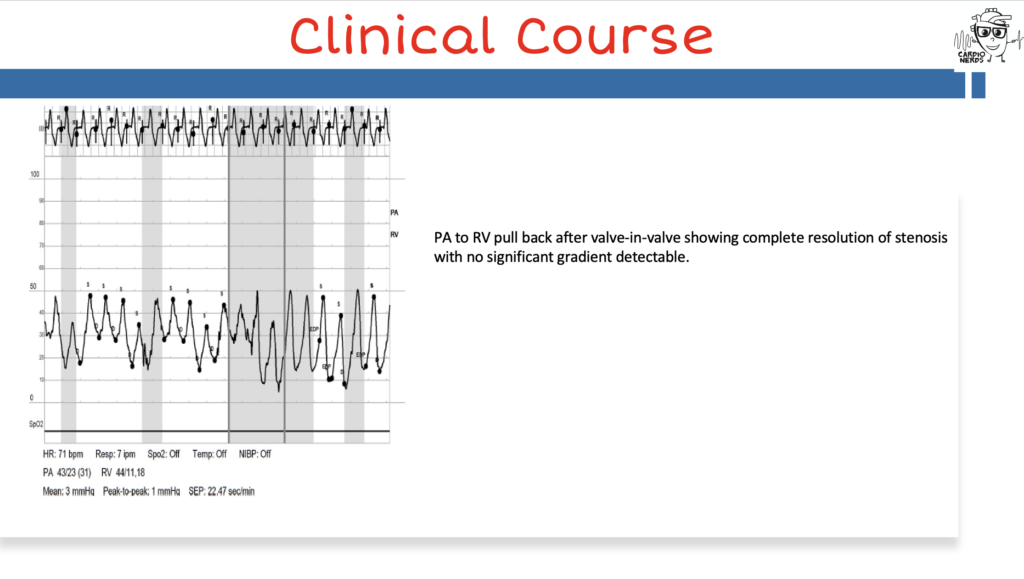
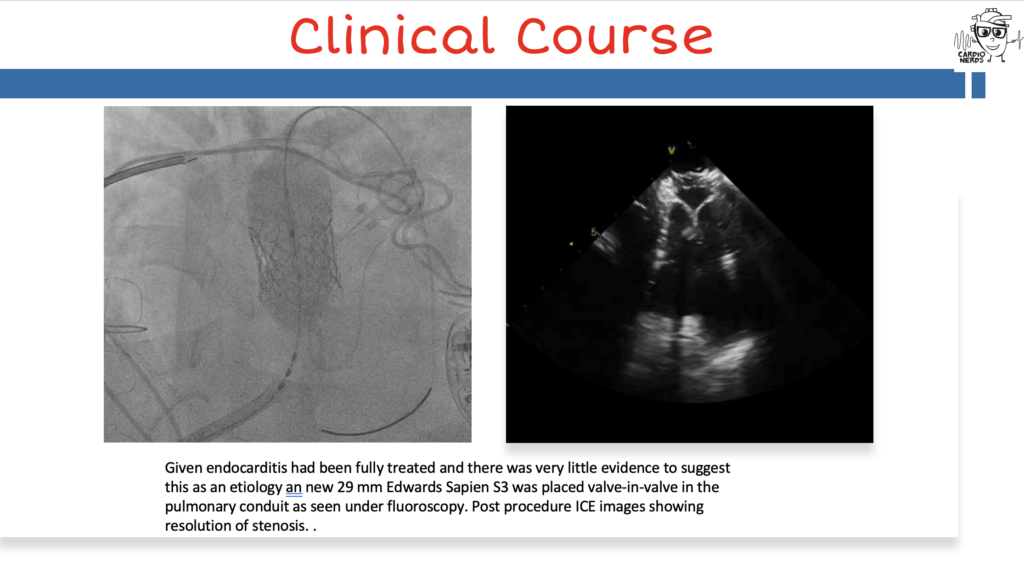
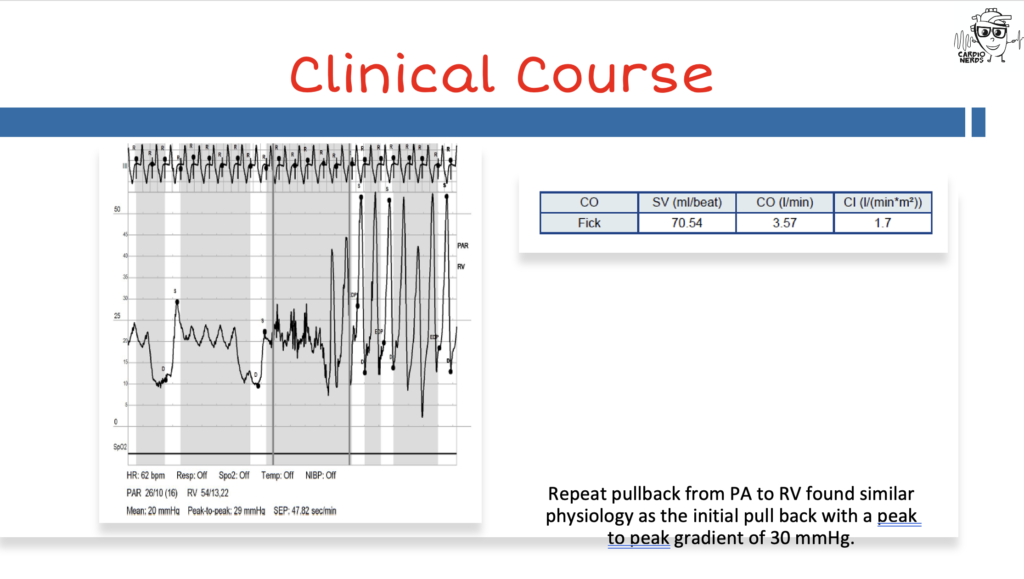
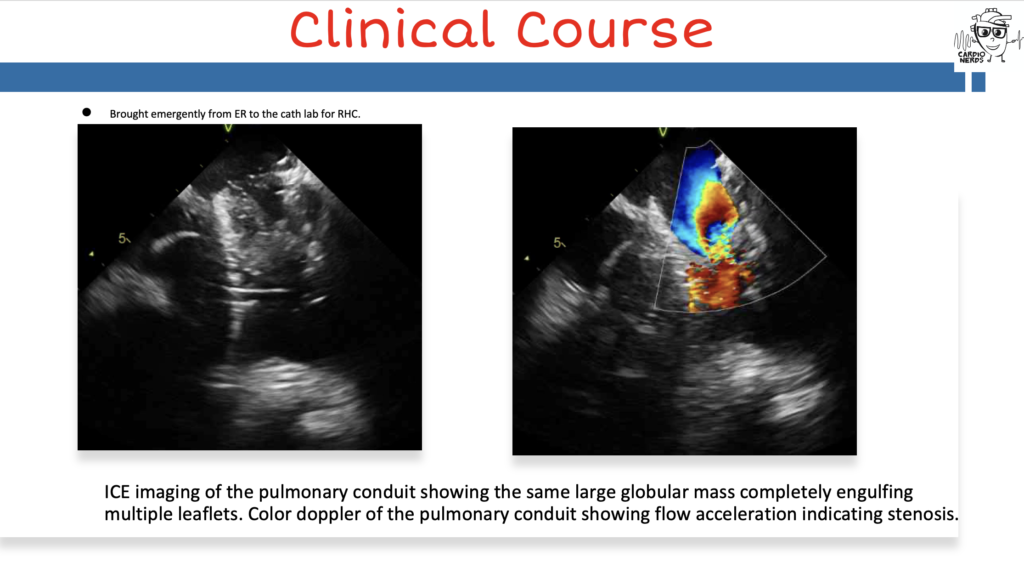
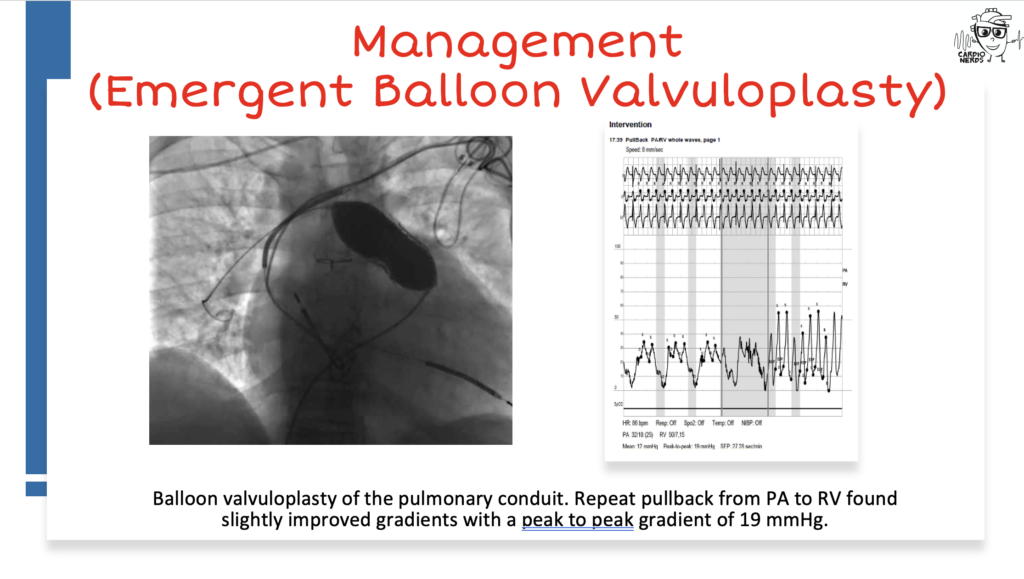
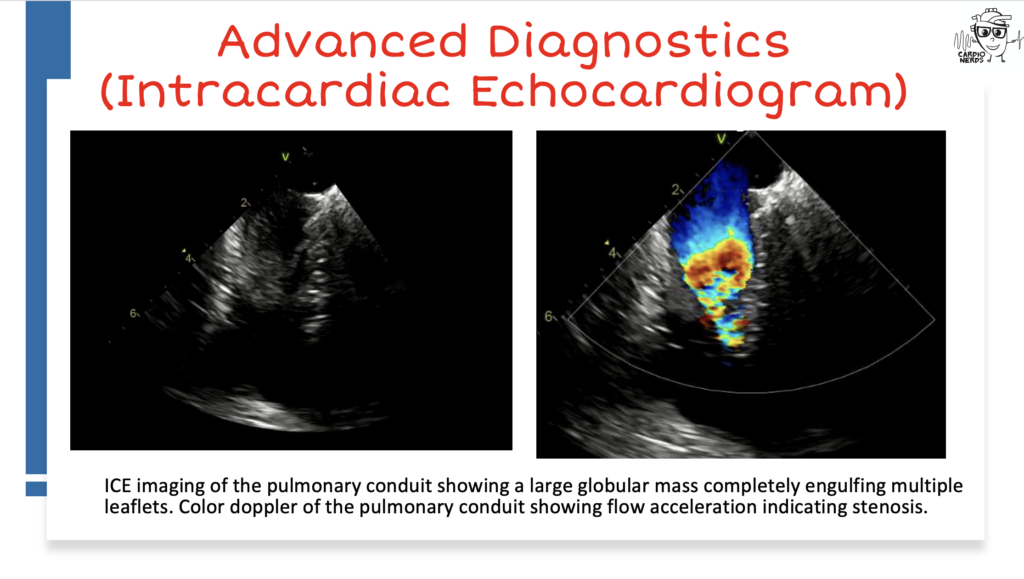
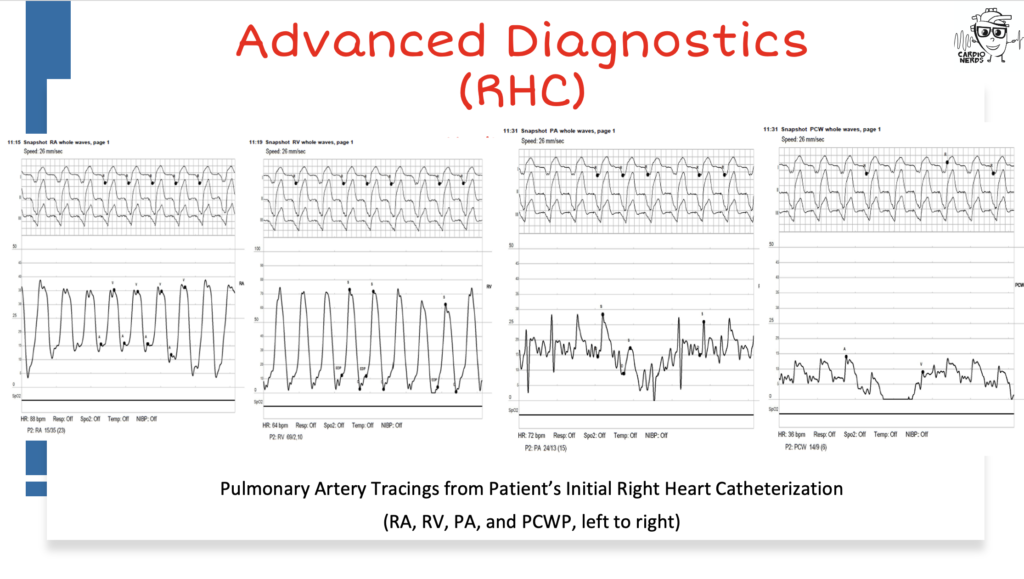
This is the case of a 42 year-old woman born with complicated Tetralogy of Fallot repair culminating in a 29mm Edwards Sapiens (ES) S3 valve placement within a pulmonary homograft for graft failure who was admitted to the cardiac ICU for progressive cardiogenic shock requiring vasopressors and inotropic support. Initial workup showed lactic acidosis, acute kidney injury, elevated NT-proBNP, and negative blood cultures. TTE showed at least moderate biventricular systolic dysfunction. She was placed on furosemide infusion, blood cultures were drawn and empiric antibiotics initiated. Right heart catheterization demonstrated elevated right sided filling pressures, blunted PA pressures with low PCWP, low cardiac index, and low pulmonary artery pulsatility index. Intracardiac echocardiography (ICE) showed a large mass within the ES valve apparatus causing restrictive valve motion with a low gradient across the pulmonic valve in the setting of poor RV function. Angiography revealed a large filling defect and balloon valvuloplasty was performed with immediate hemodynamic improvement. Blood cultures remained negative, she was gradually weaned off of inotropic and vasopressor support, and discharged. Despite empiric treatment for culture negative endocarditis and ongoing anticoagulation, she was readmitted for recurrent shock one month later at which time the pulmonic mass was revisualized on ICE. A valve-in-valve transcatheter pulmonary valve (29mm ES S3) was placed to compress what was likely pannus, with an excellent hemodynamic result and no visible mass on ICE.
“To study the phenomena of disease without books is to sail an uncharted sea, while to study books without patients is not to go to sea at all.” – Sir William Osler. CardioNerds thank the patients and their loved ones whose stories teach us the Art of Medicine and support our Mission to Democratize Cardiovascular Medicine.
US Cardiology Review is now the official journal of CardioNerds! Submit your manuscript here.
Case Media
Pearls – Obstructive Cardiogenic ShocK
- Tetralogy of Fallot is the most common cyanotic defect and can lead to long term complications after surgical repair including chronic pulmonary insufficiency, RV dysfunction, residual RVOT obstruction and branch pulmonary artery stenoses.
- Chronic RV failure may be more indicative of a structural defect and therefore require interventional or surgical management.
- Valve thrombosis, infective endocarditis and obstructive pannus formation should be considered in the differential of a patient with obstructive shock with a prosthetic valve.
- Bioprosthetic pulmonic valve obstruction may be effectively managed with balloon valvuloplasty in patients who present in acute extremis but TCPV will likely provide a more lasting result.
- While valvular gradients are typically assessed via echocardiography, invasive hemodynamics can serve as a critical adjunctive tool in its characterization.
Show Notes – Obstructive Cardiogenic ShocK
Notes were drafted by Drs. Omkar Betageri, Philip Lacombe, Cashel O’Brien, and Andrew Geissler.
What are the common therapies and management for Tetralogy of Fallot?
- Tetralogy of Fallot is the most common cyanotic defect in children beyond the age of one year
- Anatomic Abnormalities: Anterior and Superior deviation of the conal septum creating a SubAo VSD and encroachment on the RVOT. The Ao follows the conal septum anteriorly to override the VSD and RVH is a consequence of an RV chamber that is at systemic pressure.
- The need for medical intervention is dependent on the degree of RVOT obstruction, pulmonary regurgitation, and/or peripheral pulmonary artery obstruction.
- Many patients are minimally cyanotic in newborn period and clinical follow-up with elective surgical correction between 3 months and 6 months of age is a preferred approach.
- Total surgical correction typically involves placing patients on cardiopulmonary bypass, relieving right sided obstruction (sometimes utilizing trans-annular patch), and connecting left ventricular blood flow with aortic, with VSD closure.
- Hypercyanotic “Tet” spells can occur in the neonatal period when there is an acute muscular spasm in the RVOT, fall in SVR or increase in PVR to facilitate right to left shunting at the VSD. It is managed medically with a stepwise approach placing the patient in knee-chest position, administer oxygen, IV fluids and a dose of narcotics, IV beta blocker, IV phenylephrine, ECMO
- Long term complications post-surgical repair include chronic pulmonary insufficiency, RV dysfunction, residual RVOT obstruction, peripheral PA obstruction, aortic root dilation, endocarditis, arrhythmias, and sudden cardiac death.
How should we approach the management of chronic right ventricular failure?
- Briefly, RV failure can result in chamber dilatation, bowing of the interventricular septum to the LV, impairing LV stroke volume, and ultimately causing hemodynamic collapse. This is the frequently referenced “RV spiral”
- The primary step in management of RV cardiogenic shock should be to identify and reverse the primary etiology
- While patients in acute RV failure may respond well to therapies such as fluid resuscitation, inotropes and vasopressors, or inhaled nitric oxide, patients with chronic RV failure (such as in our case) are more likely to have structural defects driving their decompensation
- Chronic RV failure can result from etiologies related to preload (ASD, tricuspid and pulmonic insufficiency), afterload (pulmonic or pulmonary artery stenosis, pulmonary vascular disease, and left heart disease) or contractility (RV myopathy or ARVC).
VSD is not volume loading to RV and Eisenmenger’s would be a pressure load b/c of increased PVR and actually volume unload the RV with R to L VSD shunting.
- In acute stabilization, it is reasonable to utilize methods used to manage acute RV failure, with the understanding that interventional/surgical management will ultimately be necessary for definitive management
When should bioprosthetic valve obstruction be suspected and what is the differential for this? What is the initial workup?
- Obstruction should be suspected in any patient with a history of prosthetic valve placement who presents with a new murmur, new history of exercise intolerance, syncope/presyncope, or evidence of heart failure on exam.
- Differential diagnosis includes pannus ingrowth, thrombus, and vegetation. The anterior location of a surgically replaced RVOT/PV also makes it susceptible to compressive forces from the chest wall anteriorly and dilated Ao posteriorly, particularly in growing children. For bioprosthetic valves pannus is more common than acute thrombosis. Age of the valve, risk factors for infection, and anticoagulation status are clinical signs that may help differentiate.
- Diagnosis is typically made by transthoracic echocardiology (TTE): Increased gradients across the PV, RV hypertrophy, dilatation or dysfunction, increasing TR volume with elevated gradients from RV to RA.
- Cardiac CT or CMRI can also be helpful in characterizing the stenosis (discreet or long-segment, singular or stenoses in series).
- Invasive hemodynamic assessment in the catheterization laboratory can be especially helpful to more specifically characterize the degree and location of the obstruction as well as perform intervention (balloon, stent placement, TCPV) to relieve the obstruction. It is not uncommon that distal pulmonary artery stenting is required at the time of ballooning of the valve or valve-in-valve TCPVR.
- Lab testing sometimes performed includes INR, hemoglobin level, hemolysis labs, NT-BNP. If acute thrombosis of the bioprosthetic valve is diagnosed, a hypercoaguable work-up to include familial thrombophilia should be performed
- FDG PET may be an adjunctive tool to help evaluate for prosthetic valve endocarditis by detection of acute inflammation.
What are the indications for management of valve obstruction? What are the primary management strategies?
- As previously discussed the differential diagnosis of bioprosthetic valve obstruction includes BPVT, pannus, and vegetation. Valve intervention is indicated for symptomatic severe stenosis and treatment strategy depends on the underlying cause.
- BPVT: If stable, can trial anticoagulation therapy. If unstable immediate therapy is required which requires surgery or fibrinolytics.
- Pannus: Severe stenosis caused by soft tissue overgrowth with degeneration and calcium requires stenting open the obstructive valve in the catheterization laboratory followed by a valve-in-valve TCPV placement. It is increasingly rare that an obstructed bioprosthetic PV cannot be managed in this fashion and surgical PVR is needed. Medical therapy is ineffective in treating the underlying cause although can treat consequences from heart failure.
- Vegetation: Endocarditis with vegetation causing severe stenosis is usually treated with surgical intervention. Decisions regarding surgical indications for endocarditis are complex and a trial of medical therapy is reasonable in less severe disease.
- For native pulmonic valve obstruction many patients are amenable to balloon valvuloplasty and recurrent stenosis is rare. Patients are usually left with some degree of pulmonic insufficiency. Balloon valvuloplasty alone is rarely an effective long-term solution for bioprosthetic valve stenosis.
What is the role of right heart catheterization in valvular obstructive shock?
- Typically valve gradients are obtained by TTE in a parasternal short axis view but hemodynamic gradients measured in the cath lab can provide supportive information
- Additionally right heart catheterization can assist in the characterization of the degree of shock (through calculation of cardiac indices, pulmonary artery pulmonary index, and cardiac power output).
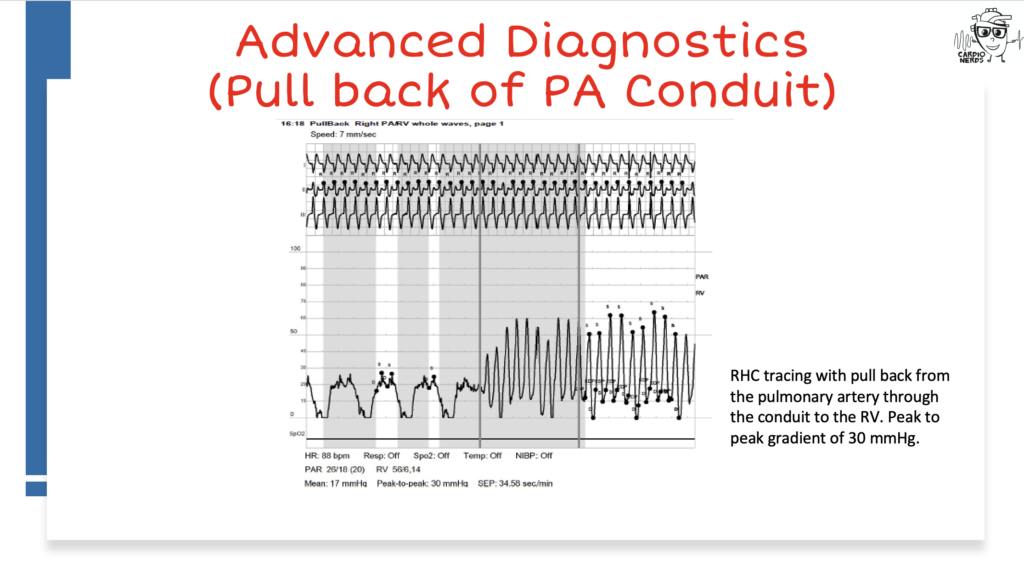
- In pulmonary stenosis, the narrowed valve creates a pressure differential between the RV and PA such that a peak pressure difference RVSP-PASP >64 mmHg is considered severe or mean difference of >35 mmHg
- As in this case, catheterization also allows for therapeutic intervention either through balloon valvuloplasty or TCPVP.
References – Obstructive Cardiogenic ShocK
- Egbe AC, Pislaru SV, Pellikka PA, et al. Bioprosthetic Valve Thrombosis Versus Structural Failure: Clinical and Echocardiographic Predictors. J Am Coll Cardiol. 2015;66(21):2285-2294. doi:10.1016/j.jacc.2015.09.022
- McElhinney DB, Zhang Y, Levi DS, et al. Reintervention and Survival After Transcatheter Pulmonary Valve Replacement. J Am Coll Cardiol. 2022;79(1):18-32. doi:10.1016/j.jacc.2021.10.031
- Nishimura RA, Carabello BA. Hemodynamics in the cardiac catheterization laboratory of the 21st century. Circulation. 2012;125(17):2138-2150. doi:10.1161/CIRCULATIONAHA.111.060319
- Otto, Catherine M et al. “2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: Executive Summary: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines.” Circulation vol. 143,5 (2021): e35-e71. doi:10.1161/CIR.0000000000000932
- Rao PS. Management of Congenital Heart Disease: State of the Art-Part II-Cyanotic Heart Defects. Children (Basel). 2019;6(4):54. Published 2019 Apr 4. doi:10.3390/children6040054
- Stout, Karen K et al. “2018 AHA/ACC Guideline for the Management of Adults With Congenital Heart Disease: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines.” Journal of the American College of Cardiology vol. 73,12 (2019): 1494-1563. doi:10.1016/j.jacc.2018.08.1028
- VARC-3 WRITING COMMITTEE et al. “Valve Academic Research Consortium 3: updated endpoint definitions for aortic valve clinical research.” European heart journal vol. 42,19 (2021): 1825-1857. doi:10.1093/eurheartj/ehaa799
- Arrigo, M., Huber, L. C., Winnik, S., Mikulicic, F., Guidetti, F., Frank, M., Flammer, A. J., & Ruschitzka, F. (2019). Right ventricular failure: Pathophysiology, diagnosis and treatment. Cardiac Failure Review, 5(3), 140–146. https://doi.org/10.15420/cfr.2019.15.2
- Kanwar, M. K., Everett, K. D., Gulati, G., Brener, M. I., & Kapur, N. K. (2022). Epidemiology and management of right ventricular-predominant heart failure and shock in the cardiac intensive care unit. European Heart Journal. Acute Cardiovascular Care, 11(7), 584–594. https://doi.org/10.1093/ehjacc/zuac063
359 episodes
Manage episode 418121214 series 2585945
Content provided by CardioNerds. All podcast content including episodes, graphics, and podcast descriptions are uploaded and provided directly by CardioNerds or their podcast platform partner. If you believe someone is using your copyrighted work without your permission, you can follow the process outlined here https://player.fm/legal.
CardioNerds Dr. Josh Saef and Dr. Tommy Das join Dr. Omkar Betageri, Dr. Andrew Geissler, Dr. Philip Lacombe, and Dr. Cashel O’Brien from the Maine Medical Center in Portland, Maine to enjoy an afternoon by the famous Portland headlight. They discuss a case of a patient who presents with obstructive cardiogenic shock. Dr. Bram Geller and Dr. Jon Donnelly provide the Expert CardioNerd Perspectives & Review segment for this episode. Dr. Maxwell Afari, the Maine Medical Center cardiology fellowship program director highlights the fellowship program. Audio editing by CardioNerds Academy Intern, student doctor Tina Reddy.
This is the case of a 42 year-old woman born with complicated Tetralogy of Fallot repair culminating in a 29mm Edwards Sapiens (ES) S3 valve placement within a pulmonary homograft for graft failure who was admitted to the cardiac ICU for progressive cardiogenic shock requiring vasopressors and inotropic support. Initial workup showed lactic acidosis, acute kidney injury, elevated NT-proBNP, and negative blood cultures. TTE showed at least moderate biventricular systolic dysfunction. She was placed on furosemide infusion, blood cultures were drawn and empiric antibiotics initiated. Right heart catheterization demonstrated elevated right sided filling pressures, blunted PA pressures with low PCWP, low cardiac index, and low pulmonary artery pulsatility index. Intracardiac echocardiography (ICE) showed a large mass within the ES valve apparatus causing restrictive valve motion with a low gradient across the pulmonic valve in the setting of poor RV function. Angiography revealed a large filling defect and balloon valvuloplasty was performed with immediate hemodynamic improvement. Blood cultures remained negative, she was gradually weaned off of inotropic and vasopressor support, and discharged. Despite empiric treatment for culture negative endocarditis and ongoing anticoagulation, she was readmitted for recurrent shock one month later at which time the pulmonic mass was revisualized on ICE. A valve-in-valve transcatheter pulmonary valve (29mm ES S3) was placed to compress what was likely pannus, with an excellent hemodynamic result and no visible mass on ICE.
“To study the phenomena of disease without books is to sail an uncharted sea, while to study books without patients is not to go to sea at all.” – Sir William Osler. CardioNerds thank the patients and their loved ones whose stories teach us the Art of Medicine and support our Mission to Democratize Cardiovascular Medicine.
US Cardiology Review is now the official journal of CardioNerds! Submit your manuscript here.
Case Media
Pearls – Obstructive Cardiogenic ShocK
- Tetralogy of Fallot is the most common cyanotic defect and can lead to long term complications after surgical repair including chronic pulmonary insufficiency, RV dysfunction, residual RVOT obstruction and branch pulmonary artery stenoses.
- Chronic RV failure may be more indicative of a structural defect and therefore require interventional or surgical management.
- Valve thrombosis, infective endocarditis and obstructive pannus formation should be considered in the differential of a patient with obstructive shock with a prosthetic valve.
- Bioprosthetic pulmonic valve obstruction may be effectively managed with balloon valvuloplasty in patients who present in acute extremis but TCPV will likely provide a more lasting result.
- While valvular gradients are typically assessed via echocardiography, invasive hemodynamics can serve as a critical adjunctive tool in its characterization.
Show Notes – Obstructive Cardiogenic ShocK
Notes were drafted by Drs. Omkar Betageri, Philip Lacombe, Cashel O’Brien, and Andrew Geissler.
What are the common therapies and management for Tetralogy of Fallot?
- Tetralogy of Fallot is the most common cyanotic defect in children beyond the age of one year
- Anatomic Abnormalities: Anterior and Superior deviation of the conal septum creating a SubAo VSD and encroachment on the RVOT. The Ao follows the conal septum anteriorly to override the VSD and RVH is a consequence of an RV chamber that is at systemic pressure.
- The need for medical intervention is dependent on the degree of RVOT obstruction, pulmonary regurgitation, and/or peripheral pulmonary artery obstruction.
- Many patients are minimally cyanotic in newborn period and clinical follow-up with elective surgical correction between 3 months and 6 months of age is a preferred approach.
- Total surgical correction typically involves placing patients on cardiopulmonary bypass, relieving right sided obstruction (sometimes utilizing trans-annular patch), and connecting left ventricular blood flow with aortic, with VSD closure.
- Hypercyanotic “Tet” spells can occur in the neonatal period when there is an acute muscular spasm in the RVOT, fall in SVR or increase in PVR to facilitate right to left shunting at the VSD. It is managed medically with a stepwise approach placing the patient in knee-chest position, administer oxygen, IV fluids and a dose of narcotics, IV beta blocker, IV phenylephrine, ECMO
- Long term complications post-surgical repair include chronic pulmonary insufficiency, RV dysfunction, residual RVOT obstruction, peripheral PA obstruction, aortic root dilation, endocarditis, arrhythmias, and sudden cardiac death.
How should we approach the management of chronic right ventricular failure?
- Briefly, RV failure can result in chamber dilatation, bowing of the interventricular septum to the LV, impairing LV stroke volume, and ultimately causing hemodynamic collapse. This is the frequently referenced “RV spiral”
- The primary step in management of RV cardiogenic shock should be to identify and reverse the primary etiology
- While patients in acute RV failure may respond well to therapies such as fluid resuscitation, inotropes and vasopressors, or inhaled nitric oxide, patients with chronic RV failure (such as in our case) are more likely to have structural defects driving their decompensation
- Chronic RV failure can result from etiologies related to preload (ASD, tricuspid and pulmonic insufficiency), afterload (pulmonic or pulmonary artery stenosis, pulmonary vascular disease, and left heart disease) or contractility (RV myopathy or ARVC).
VSD is not volume loading to RV and Eisenmenger’s would be a pressure load b/c of increased PVR and actually volume unload the RV with R to L VSD shunting.
- In acute stabilization, it is reasonable to utilize methods used to manage acute RV failure, with the understanding that interventional/surgical management will ultimately be necessary for definitive management
When should bioprosthetic valve obstruction be suspected and what is the differential for this? What is the initial workup?
- Obstruction should be suspected in any patient with a history of prosthetic valve placement who presents with a new murmur, new history of exercise intolerance, syncope/presyncope, or evidence of heart failure on exam.
- Differential diagnosis includes pannus ingrowth, thrombus, and vegetation. The anterior location of a surgically replaced RVOT/PV also makes it susceptible to compressive forces from the chest wall anteriorly and dilated Ao posteriorly, particularly in growing children. For bioprosthetic valves pannus is more common than acute thrombosis. Age of the valve, risk factors for infection, and anticoagulation status are clinical signs that may help differentiate.
- Diagnosis is typically made by transthoracic echocardiology (TTE): Increased gradients across the PV, RV hypertrophy, dilatation or dysfunction, increasing TR volume with elevated gradients from RV to RA.
- Cardiac CT or CMRI can also be helpful in characterizing the stenosis (discreet or long-segment, singular or stenoses in series).
- Invasive hemodynamic assessment in the catheterization laboratory can be especially helpful to more specifically characterize the degree and location of the obstruction as well as perform intervention (balloon, stent placement, TCPV) to relieve the obstruction. It is not uncommon that distal pulmonary artery stenting is required at the time of ballooning of the valve or valve-in-valve TCPVR.
- Lab testing sometimes performed includes INR, hemoglobin level, hemolysis labs, NT-BNP. If acute thrombosis of the bioprosthetic valve is diagnosed, a hypercoaguable work-up to include familial thrombophilia should be performed
- FDG PET may be an adjunctive tool to help evaluate for prosthetic valve endocarditis by detection of acute inflammation.
What are the indications for management of valve obstruction? What are the primary management strategies?
- As previously discussed the differential diagnosis of bioprosthetic valve obstruction includes BPVT, pannus, and vegetation. Valve intervention is indicated for symptomatic severe stenosis and treatment strategy depends on the underlying cause.
- BPVT: If stable, can trial anticoagulation therapy. If unstable immediate therapy is required which requires surgery or fibrinolytics.
- Pannus: Severe stenosis caused by soft tissue overgrowth with degeneration and calcium requires stenting open the obstructive valve in the catheterization laboratory followed by a valve-in-valve TCPV placement. It is increasingly rare that an obstructed bioprosthetic PV cannot be managed in this fashion and surgical PVR is needed. Medical therapy is ineffective in treating the underlying cause although can treat consequences from heart failure.
- Vegetation: Endocarditis with vegetation causing severe stenosis is usually treated with surgical intervention. Decisions regarding surgical indications for endocarditis are complex and a trial of medical therapy is reasonable in less severe disease.
- For native pulmonic valve obstruction many patients are amenable to balloon valvuloplasty and recurrent stenosis is rare. Patients are usually left with some degree of pulmonic insufficiency. Balloon valvuloplasty alone is rarely an effective long-term solution for bioprosthetic valve stenosis.
What is the role of right heart catheterization in valvular obstructive shock?
- Typically valve gradients are obtained by TTE in a parasternal short axis view but hemodynamic gradients measured in the cath lab can provide supportive information
- Additionally right heart catheterization can assist in the characterization of the degree of shock (through calculation of cardiac indices, pulmonary artery pulmonary index, and cardiac power output).
- In pulmonary stenosis, the narrowed valve creates a pressure differential between the RV and PA such that a peak pressure difference RVSP-PASP >64 mmHg is considered severe or mean difference of >35 mmHg
- As in this case, catheterization also allows for therapeutic intervention either through balloon valvuloplasty or TCPVP.
References – Obstructive Cardiogenic ShocK
- Egbe AC, Pislaru SV, Pellikka PA, et al. Bioprosthetic Valve Thrombosis Versus Structural Failure: Clinical and Echocardiographic Predictors. J Am Coll Cardiol. 2015;66(21):2285-2294. doi:10.1016/j.jacc.2015.09.022
- McElhinney DB, Zhang Y, Levi DS, et al. Reintervention and Survival After Transcatheter Pulmonary Valve Replacement. J Am Coll Cardiol. 2022;79(1):18-32. doi:10.1016/j.jacc.2021.10.031
- Nishimura RA, Carabello BA. Hemodynamics in the cardiac catheterization laboratory of the 21st century. Circulation. 2012;125(17):2138-2150. doi:10.1161/CIRCULATIONAHA.111.060319
- Otto, Catherine M et al. “2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: Executive Summary: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines.” Circulation vol. 143,5 (2021): e35-e71. doi:10.1161/CIR.0000000000000932
- Rao PS. Management of Congenital Heart Disease: State of the Art-Part II-Cyanotic Heart Defects. Children (Basel). 2019;6(4):54. Published 2019 Apr 4. doi:10.3390/children6040054
- Stout, Karen K et al. “2018 AHA/ACC Guideline for the Management of Adults With Congenital Heart Disease: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines.” Journal of the American College of Cardiology vol. 73,12 (2019): 1494-1563. doi:10.1016/j.jacc.2018.08.1028
- VARC-3 WRITING COMMITTEE et al. “Valve Academic Research Consortium 3: updated endpoint definitions for aortic valve clinical research.” European heart journal vol. 42,19 (2021): 1825-1857. doi:10.1093/eurheartj/ehaa799
- Arrigo, M., Huber, L. C., Winnik, S., Mikulicic, F., Guidetti, F., Frank, M., Flammer, A. J., & Ruschitzka, F. (2019). Right ventricular failure: Pathophysiology, diagnosis and treatment. Cardiac Failure Review, 5(3), 140–146. https://doi.org/10.15420/cfr.2019.15.2
- Kanwar, M. K., Everett, K. D., Gulati, G., Brener, M. I., & Kapur, N. K. (2022). Epidemiology and management of right ventricular-predominant heart failure and shock in the cardiac intensive care unit. European Heart Journal. Acute Cardiovascular Care, 11(7), 584–594. https://doi.org/10.1093/ehjacc/zuac063
359 episodes
Alla avsnitt
×Welcome to Player FM!
Player FM is scanning the web for high-quality podcasts for you to enjoy right now. It's the best podcast app and works on Android, iPhone, and the web. Signup to sync subscriptions across devices.
Similar to Cardionerds: A Cardiology Podcast
Although the world is becoming mostly sedentary, our bodies still require a wide variety of daily movements in order to work well. Many of us struggle to get regular exercise, but even that can fall short of nourishing the body from head to toe. How can we move more—a lot more—when we have sore, stiff parts and overly busy lifestyles? Join Katy Bowman M.S., biomechanist, author, and movement educator as she combines big-picture lessons on biomechanics, kinesiology, physiology, and natural hu ...
…
continue reading
Introducing the BODi® Partner Podcast, the official podcast channel devoted exclusively to BODi Partners. From archives of the BODi Wake-Up Call, I Am BODi stories, and What I Know Now success tips from seasoned Partners, this podcast is your one-stop source for personal development, business training and peer-to-peer inspiration. Ready to explode your business? Tune in regularly to our official podcast and join the ranks of those transforming their lives and the lives of others!
…
continue reading
Join expert voices from Barbell Logic and others from the world of strength for resources to help you get strong for life. Get coaching options and more educational content at barbell-logic.com.
…
continue reading
PT Inquest is an online journal club. Hosted by Jason Tuori, Megan Graham, and Chris Juneau, the show looks at an article every week and discusses how it applies to current physical therapy practice.
…
continue reading
We are often distracted in life and never really dive deep into the real foundation of self improvement, goal achieving, and wellbeing. - Join our team of experts every week as we discuss the real facets of manhood. Topics like: How to develop more self esteem, self love, deeper relationships. How to improve our wellbeing, mental toughness, resilience, and productivity. How to develop critical skills, become better leaders, expand our careers/business, create financial security and contribut ...
…
continue reading
The Art of Charm is where self-motivated people, just like you, come to learn from the company’s coaches about to how to master human dynamics, relationships, and becoming your best self with the help of Johnny and AJ, the company’s founders. Johnny and AJ bring their 11 years of coaching experience from their famous Bootcamps, where they host clients in Los Angeles from all over the world and they share their stories, best practices and themselves on this weekly podcast. Not only does The A ...
…
continue reading
Seeking a healthier emotional life? It’s time to bring a trained psychologist and mental health expert along for the ride. Dr. Monica Johnson explains the why behind complex emotions, helps you form better relationships, and guides you down the path of self-understanding.
…
continue reading
For the complete newbie or the experienced hypnotist, Brain Software with Mike Mandel is the world's most interesting, educational and fun podcast discussing hypnosis, NLP and strategies for peak performance and self improvement. Mike Mandel is a 6-time award winning hypnotist, immensely popular keynote speaker, stage performer, psychotherapist and NLP trainer. He has been doing hypnosis since he was 12 years old. Mike has an amazing ability to demystify hypnosis, teach core concepts, and te ...
…
continue reading
Welcome to Almost 30 - a supportive space to fuel your conscious evolution. Join us, LA-based best friends Krista Williams and Lindsey Simcik, for heart-centered, hilarious conversations and real, raw, impactful interviews with brilliant guests. We dive deep into topics like modern spirituality to health and wellness, aliens to entrepreneurship, social justice, and self development. With every episode, our mission is to empower you, expand what you think is possible and, make you laugh - a l ...
…
continue reading
The American healthcare system is one of the most innovative in the world. But it’s also riddled with complex challenges, such as access to affordable medications, inefficiency and administrative burdens, and communication barriers between providers. There’s clearly a better way—and at Surescripts, we have a unique sightline into what that may be. In this series, host Melanie Marcus, Chief Marketing Officer of Surescripts, sits down with today’s most inspiring and innovative leaders in healt ...
…
continue reading
Player FM - Podcast App
Go offline with the Player FM app!
Go offline with the Player FM app!