In "Hardcore History" journalist and broadcaster Dan Carlin takes his "Martian", unorthodox way of thinking and applies it to the past. Was Alexander the Great as bad a person as Adolf Hitler? What would Apaches with modern weapons be like? Will our modern civilization ever fall like civilizations from past eras? This isn't academic history (and Carlin isn't a historian) but the podcast's unique blend of high drama, masterful narration and Twilight Zone-style twists has entertained millions ...
…
continue reading
Content provided by Billy Lin, MD, Tina Lien, and BSc Pharm. All podcast content including episodes, graphics, and podcast descriptions are uploaded and provided directly by Billy Lin, MD, Tina Lien, and BSc Pharm or their podcast platform partner. If you believe someone is using your copyrighted work without your permission, you can follow the process outlined here https://player.fm/legal.
Similar to Family Medicine & Pharmacy Podcast
If you are curious about how your brain really works this is the podcast for you! Hosted by physician Dr. Ginger Campbell (2022 Podcast Hall of Fame) from 2006-2023, Brain Science explores how recent discoveries in neuroscience are unraveling the mystery of how our brain makes us human. It features conversations with leading scientists and philosophers and is "the podcast for everyone who has a brain" because Dr. Campbell makes neuroscience accessible to listeners of all backgrounds. Over 10 ...
…
continue reading
Anna Sale explores the big questions and hard choices that are often left out of polite conversation.
…
continue reading
Is your phone watching you? Can texting make you smarter? Are your kids real? Note to Self explores these and other essential quandaries facing anyone trying to preserve their humanity in the digital age. WNYC Studios is a listener-supported producer of other leading podcasts, including Radiolab, Death, Sex & Money, Snap Judgment, Here’s the Thing with Alec Baldwin, Nancy and many others. © WNYC Studios
…
continue reading
Player FM - Podcast App
Go offline with the Player FM app!
Go offline with the Player FM app!

))
Gastroenteritis in Children
Archived series ("Inactive feed" status)
When?
This feed was archived on April 19, 2019 07:10 (
Why? Inactive feed status. Our servers were unable to retrieve a valid podcast feed for a sustained period.
What now? You might be able to find a more up-to-date version using the search function. This series will no longer be checked for updates. If you believe this to be in error, please check if the publisher's feed link below is valid and contact support to request the feed be restored or if you have any other concerns about this.
Manage episode 152064811 series 1047810
Content provided by Billy Lin, MD, Tina Lien, and BSc Pharm. All podcast content including episodes, graphics, and podcast descriptions are uploaded and provided directly by Billy Lin, MD, Tina Lien, and BSc Pharm or their podcast platform partner. If you believe someone is using your copyrighted work without your permission, you can follow the process outlined here https://player.fm/legal.
Billy looked at the following guidelines to summarize the approach to a child with gastroenteritis:
UK NICE Guideline: Diarrhoea and vomiting in children under 5 (Issued: April 2009) http://guidance.nice.org.uk/cg84
CPS Guideline: Oral rehydration therapy and early refeeding in the management of childhood gastroenteritis (Posted: Nov 1, 2006) http://www.cps.ca/documents/position/oral-rehydration-therapy
History:
- onset of diarrhea and/or vomiting (gastro is sudden in onset)
- duration of vomiting and diarrhea (diarrhea 5-7 days, max 2 weeks; vomiting 1-2 days, max 3 days)
- sick contact
- pathogen exposure
- travel history
History suggestive of increased risk of dehydration:
- young age (esp <6mo)
- low birth weight infants
- >5 diarrhea in 24h
- >2 vomiting in 24h
- no oral intake
- signs of malnutrition
Think about differential diagnosis if:
- fever >38 in children younger than 3 months
- fever >39 in children older than 3 months (fever workup required)
- shortness of breath or tachypnoea
- altered conscious state
- neck stiffness
- bulging fontanelle in infants
- non-blanching rash
- blood and/or mucus in stool
- bilious (green) vomit
- severe or localised abdominal pain
- abdominal distension or rebound tenderness.
SSx of dehydration and shock
Table 1 in NICE
Increasing severity of dehydration | |||
No clinically detectable dehydration | Clinical dehydration | Clinical shock | |
Symptoms (remote and face-to-face assessments) | Appears well | Red flag Appears to be unwell or deteriorating | – |
Alert and responsive | Red flag Altered responsiveness (for example, irritable, lethargic) | Decreased level of consciousness | |
Normal urine output | Decreased urine output | – | |
Skin colour unchanged | Skin colour unchanged | Pale or mottled skin | |
Warm extremities | Warm extremities | Cold extremities | |
Signs (face-to-face assessments) | Eyes not sunken | Red flag Sunken eyes | – |
Moist mucous membranes (except after a drink) | Dry mucous membranes (except for ‘mouth breather’) | – | |
Normal heart rate | Red flag Tachycardia | Tachycardia | |
Normal breathing pattern | Red flag Tachypnoea | Tachypnoea | |
Normal peripheral pulses | Normal peripheral pulses | Weak peripheral pulses | |
Normal capillary refill time | Normal capillary refill time | Prolonged capillary refill time | |
Normal skin turgor | Red flag Reduced skin turgor | – | |
Normal blood pressure | Normal blood pressure | Hypotension (decompensated shock) |
Table 2 in CPS
TABLE 2 Clinical assessment of degree of dehydration * | ||
Mild (under 5%) | Moderate (5-10%) | Severe (over 10%) |
Slightly decreased urine output Slightly increased thirst Slightly dry mucous membrane Slightly elevated heart rate | Decreased urine output Moderately increased thirst Dry mucous membrane Elevated heart rate Decreased skin turgor Sunken eyes Sunken anterior fontanelle | Markedly decreased or absent urine output Greatly increased thirst Very dry mucous membrane Greatly elevated heart rate Decreased skin turgor Very sunken eyes Very sunken anterior fontanelles Lethargy Cold extremities Hypotension Coma |
*Some of these signs may not be present |
SSx of hypernatremic dehydration:
- jittery
- increased muscle tone
- hyperreflexia
- convulsions
- drowsiness or coma
Labs:
- No routine blood work
- Serum sodium, potassium, urea, creatinine, glucose if IV fluids or signs of hypernatremia
- Blood gas if shock suspected
Stool culture if:
- blood and/or mucus in stool
- immunocompromized
- septicemia suspected
- travel history
- diarrhea not improved by day 7
- uncertainty about diagnosis of gastroenteritis
Blood culture if antibiotic started
Watch for HUS in E. coli O157:H7
Treatment:
Figure 1 in CPS
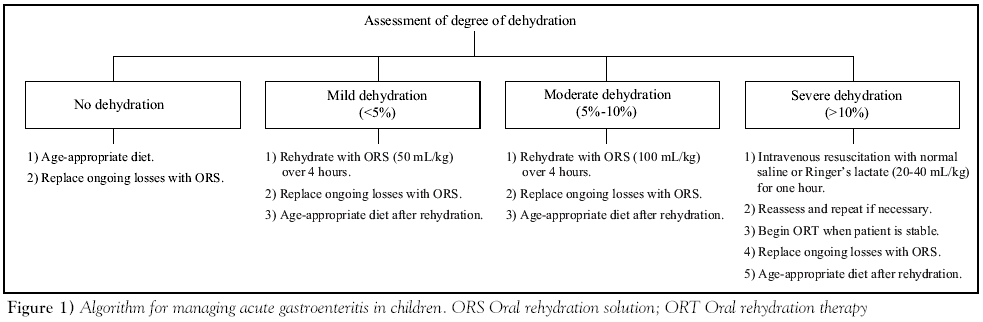
No dehydration
- continue breastfeeding and other milk feeds
- encourage fluid intake
- discourage the drinking of fruit juices and carbonated drinks, especially in those at increased risk of dehydration (see 1.2.1.2)
- offer ORS solution as supplemental fluid to those at increased risk of dehydration (see 1.2.1.2).
Dehydration
ORT
- Contraindications
- IVF indicated (shock, deterioration, persistent vomiting despite NG tube)
- paralytic ileus
- monosaccharide malabsorption
- use low-osmolarity ORS solution (240–250 mOsm/l)[5] (eg Pedialyte, Gastrolyte in Canada) for oral rehydration therapy
- give 50 ml/kg for fluid deficit replacement over 4 hours as well as maintenance fluid
- give the ORS solution frequently and in small amounts
- consider supplementation with their usual fluids (including milk feeds or water, but not fruit juices or carbonated drinks) if they refuse to take sufficient quantities of ORS solution and do not have red flag symptoms or signs (see table 1)
- plain water discouraged by CPS
- consider giving the ORS solution via a nasogastric tube if they are unable to drink it or if they vomit persistently
- monitor the response to oral rehydration therapy by regular clinical assessment
IVF
- indications:
- Shock
- a child with red flag symptoms or signs (see table 1) shows clinical evidence of deterioration despite oral rehydration therapy
- a child persistently vomits the ORS solution, given orally or via a nasogastric tube.
- Initial bolus
- 20mL/kg of NS, then another one if still shocked
- If no response to 2 boluses, consider other causes of shock. Consult PICU.
- IVF therapy
- Use NS or D5NS
- If shocked: add 100mL/kg for fluid deficit to maintenance
- If no shocked: add 50mL/kg for fluid deficit to maintenance
- Early oral rehydration recommended. Switch to ORT as early as tolerated.
- IVF in Hypernatremic dehydration
- Urgent consult to specialist
- Use NS or D5NS still
- replace slowly over 48 hours, aiming at reducing serum sodium at a rate of less than 0.5mmol/L per hour
Maintenance after rehydration
- Encourage breastfeeding, milk, and fluids
- Consider giving 5mL/kg of ORS after each large watery stool
- If dehydration recurs, restart ORT
Antibiotic indications:
- suspected or confirmed septicaemia
- extra-intestinal spread of bacterial infection
- younger than 6 months with salmonella gastroenteritis
- patient malnourished or immunocompromised with salmonella gastroenteritis
- Clostridium difficile-associated pseudomembranous enterocolitis
- giardiasis
- dysenteric shigellosis
- dysenteric amoebiasis
- cholera
Do not use antidiarrhoeal medications.
Home care
Red flags for dehydration (seek medical attention):
- appearing to get more unwell
- changing responsiveness (for example, irritability, lethargy)
- decreased urine output
- pale or mottled skin
- cold extremities
Also seek medical attention if length of illness beyond the usual course:
- diarrhoea: 5–7 days and in most children it stops within 2 weeks
- vomiting: 1 or 2 days and in most children it stops within 3 days
If not dehydrated:
- to continue usual feeds, including breast or other milk feeds
- to encourage the child to drink plenty of fluids
- to discourage the drinking of fruit juices and carbonated drinks
- plain water also discouraged by CPS
- to offer ORS solution as supplemental fluid
with clinical dehydration:
- that rehydration is usually possible with ORS solution
- premixed ORS preferred due to risk of error (CPS)
- to give 50 ml/kg of ORS solution for rehydration plus maintenance volume over a 4-hour period
- to give this amount of ORS solution in small amounts, frequently
- to seek advice if the child refuses to drink the ORS solution or vomits persistently
- to continue breastfeeding as well as giving the ORS solution
- not to give other oral fluids unless advised
- not to give solid foods.
after rehydration:
- drink plenty of their usual fluids, including milk feeds if these were stopped
- avoid fruit juices and carbonated drinks until the diarrhoea has stopped
- reintroduce the child’s usual diet
- give 5 ml/kg ORS solution after each large watery stool if you consider that the child is at increased risk of dehydration
Disease prevention
- washing hands with soap (liquid if possible) in warm running water and careful drying are the most important factors in preventing the spread of gastroenteritis
- hands should be washed after going to the toilet (children) or changing nappies (parents/carers) and before preparing, serving or eating food
- towels used by infected children should not be shared
- children should not attend any school or other childcare facility while they have diarrhoea or vomiting caused by gastroenteritis
- children should not go back to their school or other childcare facility until at least 48 hours after the last episode of diarrhoea or vomiting
- children should not swim in swimming pools for 2 weeks after the last episode of diarrhoea.
The post Gastroenteritis in Children appeared first on Family Pharm Podcast.
28 episodes
Archived series ("Inactive feed" status)
When?
This feed was archived on April 19, 2019 07:10 (
Why? Inactive feed status. Our servers were unable to retrieve a valid podcast feed for a sustained period.
What now? You might be able to find a more up-to-date version using the search function. This series will no longer be checked for updates. If you believe this to be in error, please check if the publisher's feed link below is valid and contact support to request the feed be restored or if you have any other concerns about this.
Manage episode 152064811 series 1047810
Content provided by Billy Lin, MD, Tina Lien, and BSc Pharm. All podcast content including episodes, graphics, and podcast descriptions are uploaded and provided directly by Billy Lin, MD, Tina Lien, and BSc Pharm or their podcast platform partner. If you believe someone is using your copyrighted work without your permission, you can follow the process outlined here https://player.fm/legal.
Billy looked at the following guidelines to summarize the approach to a child with gastroenteritis:
UK NICE Guideline: Diarrhoea and vomiting in children under 5 (Issued: April 2009) http://guidance.nice.org.uk/cg84
CPS Guideline: Oral rehydration therapy and early refeeding in the management of childhood gastroenteritis (Posted: Nov 1, 2006) http://www.cps.ca/documents/position/oral-rehydration-therapy
History:
- onset of diarrhea and/or vomiting (gastro is sudden in onset)
- duration of vomiting and diarrhea (diarrhea 5-7 days, max 2 weeks; vomiting 1-2 days, max 3 days)
- sick contact
- pathogen exposure
- travel history
History suggestive of increased risk of dehydration:
- young age (esp <6mo)
- low birth weight infants
- >5 diarrhea in 24h
- >2 vomiting in 24h
- no oral intake
- signs of malnutrition
Think about differential diagnosis if:
- fever >38 in children younger than 3 months
- fever >39 in children older than 3 months (fever workup required)
- shortness of breath or tachypnoea
- altered conscious state
- neck stiffness
- bulging fontanelle in infants
- non-blanching rash
- blood and/or mucus in stool
- bilious (green) vomit
- severe or localised abdominal pain
- abdominal distension or rebound tenderness.
SSx of dehydration and shock
Table 1 in NICE
Increasing severity of dehydration | |||
No clinically detectable dehydration | Clinical dehydration | Clinical shock | |
Symptoms (remote and face-to-face assessments) | Appears well | Red flag Appears to be unwell or deteriorating | – |
Alert and responsive | Red flag Altered responsiveness (for example, irritable, lethargic) | Decreased level of consciousness | |
Normal urine output | Decreased urine output | – | |
Skin colour unchanged | Skin colour unchanged | Pale or mottled skin | |
Warm extremities | Warm extremities | Cold extremities | |
Signs (face-to-face assessments) | Eyes not sunken | Red flag Sunken eyes | – |
Moist mucous membranes (except after a drink) | Dry mucous membranes (except for ‘mouth breather’) | – | |
Normal heart rate | Red flag Tachycardia | Tachycardia | |
Normal breathing pattern | Red flag Tachypnoea | Tachypnoea | |
Normal peripheral pulses | Normal peripheral pulses | Weak peripheral pulses | |
Normal capillary refill time | Normal capillary refill time | Prolonged capillary refill time | |
Normal skin turgor | Red flag Reduced skin turgor | – | |
Normal blood pressure | Normal blood pressure | Hypotension (decompensated shock) |
Table 2 in CPS
TABLE 2 Clinical assessment of degree of dehydration * | ||
Mild (under 5%) | Moderate (5-10%) | Severe (over 10%) |
Slightly decreased urine output Slightly increased thirst Slightly dry mucous membrane Slightly elevated heart rate | Decreased urine output Moderately increased thirst Dry mucous membrane Elevated heart rate Decreased skin turgor Sunken eyes Sunken anterior fontanelle | Markedly decreased or absent urine output Greatly increased thirst Very dry mucous membrane Greatly elevated heart rate Decreased skin turgor Very sunken eyes Very sunken anterior fontanelles Lethargy Cold extremities Hypotension Coma |
*Some of these signs may not be present |
SSx of hypernatremic dehydration:
- jittery
- increased muscle tone
- hyperreflexia
- convulsions
- drowsiness or coma
Labs:
- No routine blood work
- Serum sodium, potassium, urea, creatinine, glucose if IV fluids or signs of hypernatremia
- Blood gas if shock suspected
Stool culture if:
- blood and/or mucus in stool
- immunocompromized
- septicemia suspected
- travel history
- diarrhea not improved by day 7
- uncertainty about diagnosis of gastroenteritis
Blood culture if antibiotic started
Watch for HUS in E. coli O157:H7
Treatment:
Figure 1 in CPS
No dehydration
- continue breastfeeding and other milk feeds
- encourage fluid intake
- discourage the drinking of fruit juices and carbonated drinks, especially in those at increased risk of dehydration (see 1.2.1.2)
- offer ORS solution as supplemental fluid to those at increased risk of dehydration (see 1.2.1.2).
Dehydration
ORT
- Contraindications
- IVF indicated (shock, deterioration, persistent vomiting despite NG tube)
- paralytic ileus
- monosaccharide malabsorption
- use low-osmolarity ORS solution (240–250 mOsm/l)[5] (eg Pedialyte, Gastrolyte in Canada) for oral rehydration therapy
- give 50 ml/kg for fluid deficit replacement over 4 hours as well as maintenance fluid
- give the ORS solution frequently and in small amounts
- consider supplementation with their usual fluids (including milk feeds or water, but not fruit juices or carbonated drinks) if they refuse to take sufficient quantities of ORS solution and do not have red flag symptoms or signs (see table 1)
- plain water discouraged by CPS
- consider giving the ORS solution via a nasogastric tube if they are unable to drink it or if they vomit persistently
- monitor the response to oral rehydration therapy by regular clinical assessment
IVF
- indications:
- Shock
- a child with red flag symptoms or signs (see table 1) shows clinical evidence of deterioration despite oral rehydration therapy
- a child persistently vomits the ORS solution, given orally or via a nasogastric tube.
- Initial bolus
- 20mL/kg of NS, then another one if still shocked
- If no response to 2 boluses, consider other causes of shock. Consult PICU.
- IVF therapy
- Use NS or D5NS
- If shocked: add 100mL/kg for fluid deficit to maintenance
- If no shocked: add 50mL/kg for fluid deficit to maintenance
- Early oral rehydration recommended. Switch to ORT as early as tolerated.
- IVF in Hypernatremic dehydration
- Urgent consult to specialist
- Use NS or D5NS still
- replace slowly over 48 hours, aiming at reducing serum sodium at a rate of less than 0.5mmol/L per hour
Maintenance after rehydration
- Encourage breastfeeding, milk, and fluids
- Consider giving 5mL/kg of ORS after each large watery stool
- If dehydration recurs, restart ORT
Antibiotic indications:
- suspected or confirmed septicaemia
- extra-intestinal spread of bacterial infection
- younger than 6 months with salmonella gastroenteritis
- patient malnourished or immunocompromised with salmonella gastroenteritis
- Clostridium difficile-associated pseudomembranous enterocolitis
- giardiasis
- dysenteric shigellosis
- dysenteric amoebiasis
- cholera
Do not use antidiarrhoeal medications.
Home care
Red flags for dehydration (seek medical attention):
- appearing to get more unwell
- changing responsiveness (for example, irritability, lethargy)
- decreased urine output
- pale or mottled skin
- cold extremities
Also seek medical attention if length of illness beyond the usual course:
- diarrhoea: 5–7 days and in most children it stops within 2 weeks
- vomiting: 1 or 2 days and in most children it stops within 3 days
If not dehydrated:
- to continue usual feeds, including breast or other milk feeds
- to encourage the child to drink plenty of fluids
- to discourage the drinking of fruit juices and carbonated drinks
- plain water also discouraged by CPS
- to offer ORS solution as supplemental fluid
with clinical dehydration:
- that rehydration is usually possible with ORS solution
- premixed ORS preferred due to risk of error (CPS)
- to give 50 ml/kg of ORS solution for rehydration plus maintenance volume over a 4-hour period
- to give this amount of ORS solution in small amounts, frequently
- to seek advice if the child refuses to drink the ORS solution or vomits persistently
- to continue breastfeeding as well as giving the ORS solution
- not to give other oral fluids unless advised
- not to give solid foods.
after rehydration:
- drink plenty of their usual fluids, including milk feeds if these were stopped
- avoid fruit juices and carbonated drinks until the diarrhoea has stopped
- reintroduce the child’s usual diet
- give 5 ml/kg ORS solution after each large watery stool if you consider that the child is at increased risk of dehydration
Disease prevention
- washing hands with soap (liquid if possible) in warm running water and careful drying are the most important factors in preventing the spread of gastroenteritis
- hands should be washed after going to the toilet (children) or changing nappies (parents/carers) and before preparing, serving or eating food
- towels used by infected children should not be shared
- children should not attend any school or other childcare facility while they have diarrhoea or vomiting caused by gastroenteritis
- children should not go back to their school or other childcare facility until at least 48 hours after the last episode of diarrhoea or vomiting
- children should not swim in swimming pools for 2 weeks after the last episode of diarrhoea.
The post Gastroenteritis in Children appeared first on Family Pharm Podcast.
28 episodes
All episodes
×Welcome to Player FM!
Player FM is scanning the web for high-quality podcasts for you to enjoy right now. It's the best podcast app and works on Android, iPhone, and the web. Signup to sync subscriptions across devices.
Similar to Family Medicine & Pharmacy Podcast
In "Hardcore History" journalist and broadcaster Dan Carlin takes his "Martian", unorthodox way of thinking and applies it to the past. Was Alexander the Great as bad a person as Adolf Hitler? What would Apaches with modern weapons be like? Will our modern civilization ever fall like civilizations from past eras? This isn't academic history (and Carlin isn't a historian) but the podcast's unique blend of high drama, masterful narration and Twilight Zone-style twists has entertained millions ...
…
continue reading
If you are curious about how your brain really works this is the podcast for you! Hosted by physician Dr. Ginger Campbell (2022 Podcast Hall of Fame) from 2006-2023, Brain Science explores how recent discoveries in neuroscience are unraveling the mystery of how our brain makes us human. It features conversations with leading scientists and philosophers and is "the podcast for everyone who has a brain" because Dr. Campbell makes neuroscience accessible to listeners of all backgrounds. Over 10 ...
…
continue reading
Anna Sale explores the big questions and hard choices that are often left out of polite conversation.
…
continue reading
Is your phone watching you? Can texting make you smarter? Are your kids real? Note to Self explores these and other essential quandaries facing anyone trying to preserve their humanity in the digital age. WNYC Studios is a listener-supported producer of other leading podcasts, including Radiolab, Death, Sex & Money, Snap Judgment, Here’s the Thing with Alec Baldwin, Nancy and many others. © WNYC Studios
…
continue reading
Player FM - Podcast App
Go offline with the Player FM app!
Go offline with the Player FM app!



