
))
REBEL Core Cast 116.0 – Achilles Tendon Rupture
Manage episode 397396669 series 3435728
Content provided by Salim R. Rezaie, MD, Salim R. Rezaie, and MD. All podcast content including episodes, graphics, and podcast descriptions are uploaded and provided directly by Salim R. Rezaie, MD, Salim R. Rezaie, and MD or their podcast platform partner. If you believe someone is using your copyrighted work without your permission, you can follow the process outlined here https://player.fm/legal.

 Take Home Points
Take Home Points
- Achilles tendon rupture is a clinical diagnosis. The Thompson Test should be applied in all suspected cases.
- Remember to brace or splint a rupture, even if suspected, in the resting equinus position for optimal healing and prevention of further injury.
- Schedule follow up with orthopedics within 1 week for discussion of operative management vs early rehab protocols.
REBEL Core Cast 116.0 – Achilles Tendon Rupture
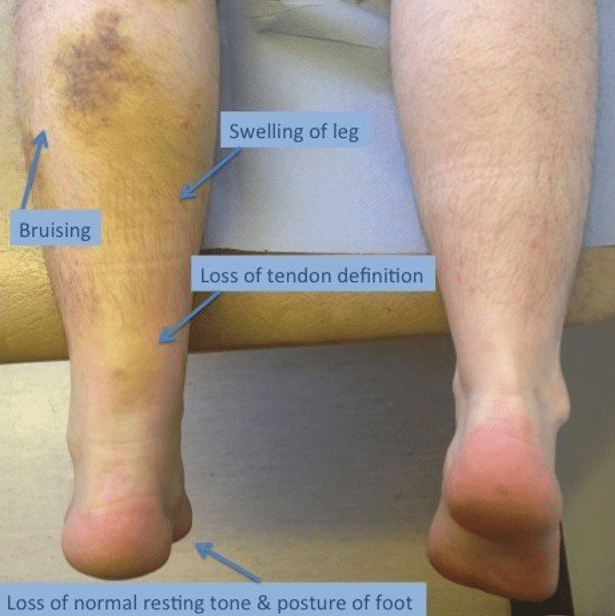
Physical Exam
- May have palpable gap or deformity in region of tendon.
- Weakness with plantar flexion.
- Increased resting ankle dorsiflexion on affected side in prone position with knees bent .
- Usually in absence of bony tenderness unless accompanied by other injury
- Thompson Test (video)
- Place the patient in the prone position, with feet hanging over the end of a stretcher or table. If patient is not able to lay down/there are no stretchers, the patient can kneel on a stool or chair
- Squeeze the calf of the normal limb. You will notice the squeeze will cause the ankle to plantarflex appropriately
- Squeeze the calf of the limb with the suspected Achilles tendon rupture. You will notice the squeeze will cause no motion if there is a full rupture/tear, and diminished motion if there is a partial tear
- Performance Characteristics (Garras 2012)
Sensitivity | Specificity | (+) LR | (-) LR |
96-100% | 93-100% | 13.7 | 0.04 |
Imaging
- X-Rays
- Used to rule out other or concurrent pathology
- May show soft tissue swelling and destruction of pre-Achilles fat pad (Kager’s Fat Pad)
- Findings are non-specific as tear of tendon unable to be visualized
- Ultrasound
- Ultrasound is helpful if obvious findings present and to distinguish between partial vs complete tears, however only around 50% sensitive for detecting only partial tears (Kayser 2005)
- MRI
- Gold-standard imaging modality
- Rarely, if ever, necessary in the ED
- Used for equivocal physical exam/alternate imaging findings or for assessing the severity of the tear for possible operative management
- Findings
- A full-thickness tear often shows a tendinous gap filled with edema or blood
- Complete rupture shows retraction of tendon ends
ED Management
-
- Provide analgesia
- Tendon stabilization in an optimal healing position
- Functional bracing/splinting in resting equinus/talipus equinus
- AO splint/brace in 20 degrees of plantar flexion for 4-6 weeks (may use tall CAM boot with 20 degrees wedge inserts)
- All patients should be non-weightbearing
- Any weight-bearing can convert a partial tear to a complete tear
- Maintain non-weightbearing status until see orthopedics (within 1 week)
- After evaluation by orthopedics, early weight-bearing and early ROM exercises yield better outcomes (can be as early as 2 weeks)
- Referral to rehab warranted to improve plantar flexion and decrease risk of re-rupture
- ED Ortho consultation: patients with open wounds in the area of trauma, or with concomitant fractures
- Operative Management is usually reserved for acute ruptures (approximately <6 weeks) of full thickness with large tendon gaps, failed conservative treatment of partial thickness tears, or high performance athletes
- These cases will be determined during follow up with orthopedics and may warrant outpatient MRI to assess severity of tear
Prognosis
-
- For conservative management, there is no significant difference in plantar flexion strength (Willits, 2010)
- Some increased risk of re-rupture compared to operative management, although review of evidence shows that this may not be significant if patients used structured, accelerated rehab protocol.
- Protocol includes initially non-weightbearing cast with the foot in equinus position as described above, then transitioned to a pneumatic walker with elevated heels (elevation gradually reduced biweekly), and physical therapy to improve gait, strength, and mobility. (Wallace 2011)
- If addressed early and appropriately, most patients have good self-reported long-term outcomes regardless of the treatment modality
Links
Orthobullets: Achilles Tendon Rupture
Resources:
- Sheth U et al. The epidemiology and trends in management of acute Achilles tendon ruptures in Ontario, Canada: a population-based study of 27,607 patients. Bone Joint J. 2017; 99-B(1): 78-86. PMID: 28053261
- Chiodo CP, Wilson MG. Current Concepts Review: Acute Ruptures of the Achilles Tendon. Foot Ankle Int 2006; 27(4): 305-13. PMID: 16624224
- Leppilahti J, Orava S. Total Achilles tendon rupture. A review. Sports Med. 1998; 25(2): 79-100. PMID: 9519398
- Kayser R et al. Partial rupture of the proximal Achilles tendon: a differential diagnostic problem in ultrasound imaging. Br J Sports Med. 2005; 39(11): 838-42. PMID: 16244194
- Margetic P et al. Comparison of ultrasonographic and intraoperative findings in Achilles tendon rupture. Coll Antropol. 2007; 31:279-284. PMID: 17598414
- Garras DN et al. MRI is Unnecessary for Diagnosing Acute Achilles Tendon Ruptures: Clinical Diagnostic Criteria. Clin Orthop Relat Res 2012; 470(8): 2268-2273. PMID: 22538958
- Willits K et al. Operative versus nonoperative treatment of acute Achilles tendon ruptures: a multicenter randomized trial using accelerated functional rehabilitation .J Bone Joint Surg Am. 2010; 92(17): 2767-75. PMID: 21037028
- Wallace RG et al. The non-operative functional management of patients with a rupture of the tendo Achillis leads to low rates of re-rupture. J Bone Joint Surg Br 2011; 93(10):1362-6. PMID: 21969435
- Erickson BJ. Is Operative Treatment of Achilles Tendon Ruptures Superior to Nonoperative Treatment? Orthop J Sports Med. 2015; 3(4): PMID: 26665055
Post Peer Reviewed By: Salim R. Rezaie, MD (Twitter/X: @srrezaie)
The post REBEL Core Cast 116.0 – Achilles Tendon Rupture appeared first on REBEL EM - Emergency Medicine Blog.
15 episodes



