PT Inquest is an online journal club. Hosted by Jason Tuori, Megan Graham, and Chris Juneau, the show looks at an article every week and discusses how it applies to current physical therapy practice.
…
continue reading
Content provided by Stacey Richter. All podcast content including episodes, graphics, and podcast descriptions are uploaded and provided directly by Stacey Richter or their podcast platform partner. If you believe someone is using your copyrighted work without your permission, you can follow the process outlined here https://player.fm/legal.
Similar to Relentless Health Value™
A daily dose of irreverent, offbeat, and informative takes on business & tech news. Hosted by Jon Weigell, Juliet Bennett Rylah, Mark Dent, Ben Berkley, Sara Friedman and Rob Litterst from The Hustle.
…
continue reading
Bloomberg Daybreak delivers today's top stories, with context, in just 15 minutes. Get informed from Bloomberg's 2,700 journalists and analysts in 120 countries.
…
continue reading
The economy and the markets are "under surveillance" as we cover the latest in finance, economics and investment. Listen to Jonathan Ferro, Lisa Abramowicz and Annmarie Hordern for the top interviews from Bloomberg Surveillance Television. And join Tom Keene and Paul Sweeney for the best conversations from Bloomberg Surveillance Radio. Watch Surveillance TV LIVE each mornings: http://bit.ly/3P7nstQ. Watch Surveillance Radio LIVE weekday mornings: http://bit.ly/3vTiACF.
…
continue reading
The American healthcare system is one of the most innovative in the world. But it’s also riddled with complex challenges, such as access to affordable medications, inefficiency and administrative burdens, and communication barriers between providers. There’s clearly a better way—and at Surescripts, we have a unique sightline into what that may be. In this series, host Melanie Marcus, Chief Marketing Officer of Surescripts, sits down with today’s most inspiring and innovative leaders in healt ...
…
continue reading
Tempers fly as the newsmakers of the week face-off in this award-winning show. Anchored by Sanket Upadhyay, this weekly program has politicians battlling wits with a live audience.
…
continue reading
Join Larry Mantle weekdays for lively and in-depth discussions of Los Angeles and Southern California news, politics, science, entertainment, the arts and more. More AirTalk at www.kpcc.org.
…
continue reading
Brilliant solutions to the world’s problems. We meet people with ideas to make the world a better place and investigate whether they work.
…
continue reading
A handpicked article read aloud from the latest issue of The Economist. Published weekdays from Monday to Thursday. If you’re already a subscriber to The Economist, you’ll have full access to all our shows as part of your subscription. For more information about Economist Podcasts+, including how to get access, please visit our FAQs page here https://myaccount.economist.com/s/article/What-is-Economist-Podcasts.
…
continue reading
Introducing the BODi® Partner Podcast, the official podcast channel devoted exclusively to BODi Partners. From archives of the BODi Wake-Up Call, I Am BODi stories, and What I Know Now success tips from seasoned Partners, this podcast is your one-stop source for personal development, business training and peer-to-peer inspiration. Ready to explode your business? Tune in regularly to our official podcast and join the ranks of those transforming their lives and the lives of others!
…
continue reading
Player FM - Podcast App
Go offline with the Player FM app!
Go offline with the Player FM app!

))
EP442: A Short Rumination on Saving Money, Except Not Saving Money. Oncology Side Effect Management as a Case Study, With Andreas Mang
Manage episode 425889353 series 2701020
Content provided by Stacey Richter. All podcast content including episodes, graphics, and podcast descriptions are uploaded and provided directly by Stacey Richter or their podcast platform partner. If you believe someone is using your copyrighted work without your permission, you can follow the process outlined here https://player.fm/legal.
This week, I’m gonna play an outtake, I guess it could be called, from the show with Andreas Mang from Blackstone that we wound up cutting for reasons of time and topic; but it’s been on my mind ever since. So, here’s this clip; and then I’m gonna invite you to partake in my ruminations because they hit the trifecta of employers and taxpayers and patients themselves getting taken for a ride from a cost perspective, while at the same time, patients are harmed. And the whole thing is so shortsighted.
Anyway, here’s the clip that started my downward spiral into … what’s the medical mental health term when you can’t stop rehashing something? Here’s the clip.
So, what is the number one … I gave it to you already, but I’ll just repeat it. Number one reason for readmissions, I think universally, if you looked at any health plan—and readmissions are bad, right? Bad quality and really expensive because something you went in for and came out, you’re back in, and it’s probably pretty bad. But the number one root cause of readmissions is dehydration associated with chemotherapy. Think how silly that is. Dehydration should not be the reason. So, you’re getting chemo, you’re feeling sick, you can’t keep down fluids, you’re vomiting, and so, you end up back in the hospital.
Well, guess what? There’s medications for that. Real simple, easy-to-take meds that’s the nausea so you can keep down fluids so you don’t get dehydrated. So, what have we done? In our world, on our platform—and health plans have tried to do this too, and they’ve done a reasonable job with their nurses and care managers—but like, in our world, we have an oncology trained nurse that is on your hip through your treatment as you go from Dr. Jones to Dr. Richter to Dr. Mang to doc, right? And none of us are talking to each other.
And so … but you have Nurse Sally on your hip talking to you whenever you want. At a minimum, they’re checking in with you, maybe it’s daily, during different bouts of treatment. “Hey, how you feeling today, Andreas?” I can’t keep down my … I’m nauseous. I’m not drinking anything. “Oh, let me call your doctor, let me get you a med, let’s get you that script that’s gonna suppress your nausea and be able to keep down fluids. You won’t end up back in the hospital.” Pretty simple solution, right?
So that was Andreas Mang, and go back and listen to the whole episode 419 about the whole way health benefits have become financialized in ways that CFOs and CEOs and boards of directors may want to be aware of—it’s not just people downstairs or in the warehouse who get cancer, after all—but also for all of the reasons which Andreas covers really well in that earlier episode. Andreas, by the way, is senior managing director at Blackstone and CEO of Equity Healthcare at Blackstone.
Let’s get this party started with a Tweet from Mark Lewis, MD. Mark Lewis is an oncologist, and he tweeted:
Dear insurance companies,
Anti-nausea medications signify one of the greatest advances in oncology.
Chemotherapy has to be effective, yes, but it has to be tolerable too. My patients risk getting sick every cycle. Please help me help them. It’s never been more important.
Then here’s what Celena Latham wrote in response to this Mark Lewis, MD, tweet. And if you go hunting around on Twitter or X or Facebook, you can find literally thousands of others saying the same basic thing.
Celena writes, “I fight with my insurance company all the time. They are happy to pay for my $10k-a-month chemo drug. But the $10-a-day nausea med is restricted. I am only allowed a 21-day supply at a time. The supply given is not enough.”
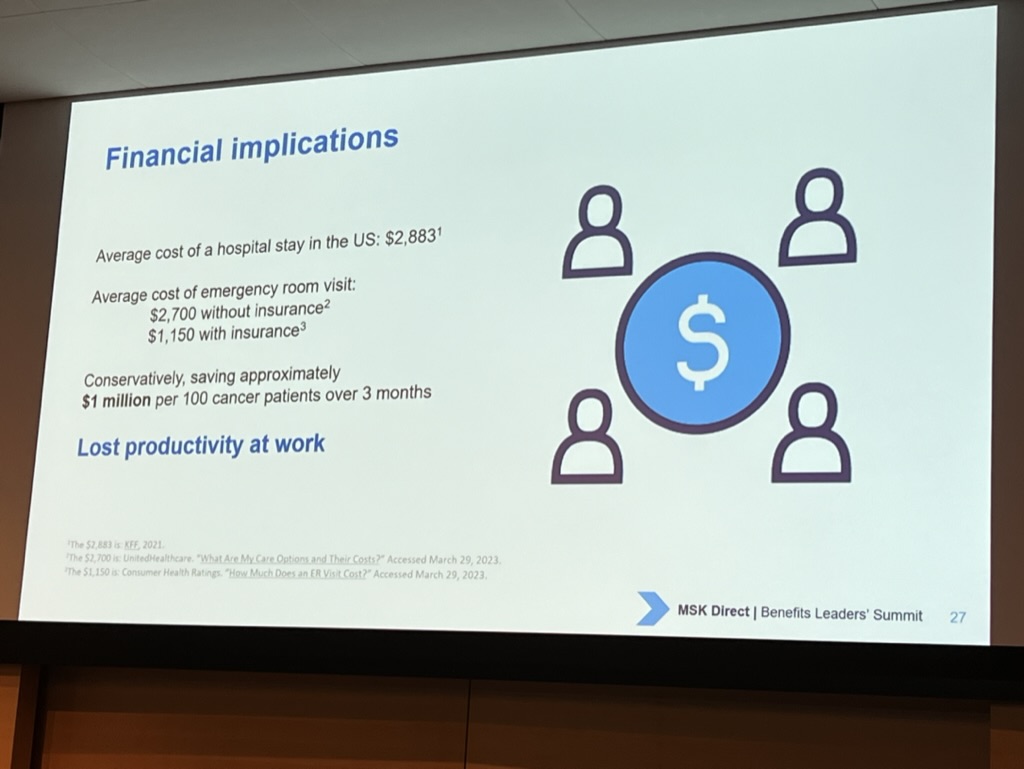
I was keeping all of this in the back of my mind when, in May, I was at the Memorial Sloan Kettering MSK Direct Day. And I heard a talk from Jun Mao, MD, that puts a lot of this in context. Dr. Mao presented a slide. Turns out, studies show, you can save $1 million per 100 cancer patients over three months by doing what’s called integrative oncology. And a big part of that, or a part of that, is managing treatment side effects like nausea and vomiting and thus keeping patients out of the ER for dehydration.
Thanks, by the way, very much to Greg Green and Emily Kauff for inviting me to that event. It was great.
Now, is this whole “hey, let’s manage oncology side effects” line of thinking some sort of breaking science? Let me refer you to a show I did with Ethan Basch, MD (EP157) in 2017. That was seven years ago. It is entitled “Major Improvements in Oncology Outcomes When Patients Self-Report Symptoms.”
In that interview, you can hear Dr. Basch talk about how he and his colleagues found that by doing things like managing side effects like nausea, patient survival time improved about five months. Those drugs that cost hundreds of thousands of dollars that are coming out, those immunology agents, many of them do not increase survival time this long.
So, not only are we talking about saving money here by managing side effects, but wait, there’s more. Survival time improves by an astounding amount, really, comparatively. We also had on the show in 2020 Nadine Jackson McCleary, MD, MPH, BSN, from Dana Farber and Harvard Medical School (EP254). She was talking about this. Oh, and also Glenn Sabin from FON Consulting in episode 233.
So, this is not news is the bottom line. And all of these kinds of facts and figures have been running through my mind while I’ve been ruminating over that outtake with Andreas Mang that I just played. Now let me get into the kind of the whys and the wherefores that I just really can’t stop rehashing.
First off, let’s just keep in mind, PBMs (pharmacy benefit managers) often have but one incentive, maybe but one job, depending on who you talk to and from where. And that one job is to lower drug costs, at least for themselves. Right now, some PBM is busy regaling their employer client about how much money they saved.
But let’s just say the quiet part out loud. In the oncology part of that spreadsheet, if the PBM restricts access to nausea meds, the employer will have lower PBM costs and higher medical costs. Let’s say the nausea med costs $5 a month, or even $1430 a month, which is the cost for a four-drug nausea and vomiting prophylaxis regimen, as per the NIH study I just read.
So, here’s me comparing that $5 to $1430 a month to the aforementioned $1 million saved on 100 cancer patients over three months stat that’s $3300 a month per patient. So, you know, PBM saves five bucks, a few hundred bucks, maybe even 1500 beans on the high end. And we spend $3300 on medical costs.
In this case, the downstream impact is also not gonna take years to accrue, so everybody wonders if they’re footing the bill for Medicare or somebody else who’s gonna receive that downstream cost savings. No, this is pretty immediate balloon squeezing, I would say. Right? Cancer patient has untreated nausea and vomiting. Cancer patient winds up in the ER.
Dan Mendelson talked about this in episode 435, by the way. He said—extremely crisply, I would add—plan sponsors gotta look at the total cost of care (ie, PBM, pharmacy spend, and medical spend together).
So that’s my first point to ponder, just the vital nature of aggregating PBM and medical data into a database of total costs. Which means that anybody trying to do population health can do their own math as opposed to relying on vendors to calculate their own “savings,” which anyone who has ever hired a point solution knows has the potential to not go well because it could enable somebody to “save” money in one place and cost a whole lot of money elsewhere.
Cora Opsahl also talks along these lines very compellingly in episode 372. She says if your data analyst can’t find savings opportunities—and, by the way, data analysts looking at the full dataset, such as the nausea example—but if they can’t find savings equivalent to their salary, then you have the wrong analyst, not a superior health plan.
Al Lewis talked about this also in great detail in episode 331. And furthermore, if we need one, I was also talking to Shawn Gremminger the other day from the National Alliance; and he said this exact same thing. Aggregate your data so you can see the total cost of care. Do your own math.
And look, I think everybody is saying this exact same thing because at least one goal is to spend less overall, not spend less on your way to spending more. Because that doesn’t count. This matters if you’re actually gonna succeed in cutting out waste and spend. But I might also scramble out on a limb and suggest that in probably a lot of instances, if you identify something that costs less in the short term but drives up the total cost of care—especially when that total cost of care is going up in a relatively short-term period—and if you know this and correct it by just spending a little bit more going in so that you spend less overall, you probably just fixed what is very likely a problem for patients in patient health. Feel free to agree or disagree on that point, but I bet I’m right.
That’s my first rumination. Just how this nausea from chemo is a great example of the why with you got to know the total cost of care.
My second rumination is just the whole thing with value-based drug purchasing or even medical purchasing, as opposed to cost-containment efforts that could spike costs elsewhere and/or cause a lot of presenteeism and absenteeism while the PBM vendor or maybe even the ASO (administrative services organization) or some provider organization gets a prize for controlling trend in the very short term, probably. Nina Lathia, RPh, MSc, PhD, talks about this in episode 426, and also Barbara Wachsman (EP430).
So, second point, having a value mindset when purchasing is a thing. Look, I’m just gonna state for the record that Blackstone knows how money works. And they have calculated, I would trust, that it is cheaper, at least for their populations, it is cheaper to manage chemo side effects than to not manage them. Or even worse, to restrict access to needed medications.
Which leads me to the third thing I’m thinking about as I consider how it can be that chemo side effects like nausea can possibly, in this day and age, go untreated or undertreated or undermanaged. I was talking to John Lee, MD (EP438) the other day; and he was talking about getting blood pressure readings from heart failure patients. (But trust me, I will bring this back to oncology patients left to their own devices in just one sec.) So, it turns out, the best way to get blood pressure readings from heart failure patients at home to make sure they don’t wind up in the ER and readmitted is have a nurse call them at home and ask them what their blood pressure is.
Works actually a lot better than any fancy stuff you might have been thinking of, but most provider organizations won’t do any dialing for blood pressure readings because they don’t get paid for it. And I’m pointing fingers all over the place and nowhere right now, but consider this blood pressure reading case study in the realm of managing oncology side effects like nausea.
For any given patient population, who is doing this side effect management? Does anyone know? Is anyone getting paid for it? And if no one is getting paid directly, then which hospitals are taking dollars they’re earning from buy and bill, which could be four to six times the cost of some of these oncology drugs (ie, a lot of money, lots of zeros)? Listen to episode 370 with Erik Davis and Autumn Yongchu for just how many zeros and how they’re doing it. But which oncology centers are taking these tens of thousands of dollars earned on the backs of buy and bill and using this money to run integrative oncology programs or manage side effects, like nausea?
A few do, don’t get me wrong; many do not. Or they don’t do nearly the stuff required as per the studies which demonstrate actual patient results. Like, you have to be collecting PROMs (patient-reported outcome measures) etc.
Tom X. Lee, MD, talks about this also in an upcoming show, this whole idea of having a value mindset and considering what good for patients looks like and then figuring out within current payment models how to make this happen so that patients get better care.
But also—and this can’t be understated—doctors and clinicians are happier and not morally fatigued by an obvious failure to, you know, not have patients spend the last three nights curled up on a towel under their toilet before heading to the ER to get hooked up to an IV. So that’s my point three rumination.
Fee for service (FFS) does not pay or pay adequately for stuff like making sure chemo patients, who, a lot of the time, will have side effects that can be costly. FFS does not pay to ensure they are proactively well managed. What FFS will pay for is waiting for the patients to fall off the cliff instead of preventing them from falling, as Darrell Moon often says. I guess this is the story of FFS, but this one, this whole nausea case study, pretty quickly has accruing costs financially and also from an employee emotional and physical impact standpoint.
So, back to that Andreas Mang quote, it seems like he and his team have concluded there could be a ton of variability in care. Providers may or may not have a value mindset and sufficient operational chops and may or may not choose to use dollars they earn off drugs or other services to do meaningful things that they may or may not get compensated for. This feels like something payers should be cognizant of because most employers don’t have resources Blackstone has to stand up their own nurse program when providers fail here.
And there also could be probably a pretty big equity consideration in the mix at the same time. But just point three, fee for service doesn’t pay for stuff like this. It’s gonna be up to a provider to choose to do it or not to do it. And all of that is a consideration for employers.
Here’s my last point I’m pondering, number four. And it also concerns what’s going on in or about oncology centers themselves. I thought of this while moderating a panel at the recent thINc Conference last month, and on this panel was Buck Poropatich from Lyft Healthcare. He said something fascinating. He said there’s two business cases for a health system to pay for transportation. And again, I’m gonna talk about transportation for a sec, but this is relevant to our oncology side effect management case study here.
So, two transportation case studies or two transportation business models: One is the value-based care arrangement business model, but let’s not talk about that one because it’s very obvious to most how dealing with social drivers of health is key when you are getting capitated payments to manage patient populations when you are, in fact, responsible for downstream costs of care; so, let’s just set aside the value-based care business model for transportation.
The business case I was fascinated by, though, is the fee-for-service business case for a hospital or provider organization to pay for transportation. It’s because no-shows are really expensive from a lost revenue perspective, and a lot of times the reason patients no-show is because they do not have transportation.
Or another use case is getting a patient discharged promptly to turn over a bed when the patient can’t get a ride home. If a health system is savvy enough to do the math, it might wind up being a profitable endeavor to pay for transportation for patients who need it. I started pondering this in the context of oncology center/provider organizations doing side effect management properly.
Is there an FFS/buy and bill “why” to stand up some of the care flows and do the outreaches and apps really well that are all necessary to do side effect management right? Is there a business case to do all of this in a fee-for-service environment?
Short answer: I don’t know, but I keep seeing studies showing that when side effects aren’t managed, courses of therapy are shortened (to the patient’s detriment we’re talking now in this use case) or doses are lowered or patients die prematurely. You would think that if someone at an oncology center was able to and did calculate the lost revenue from any or all of these downstream impacts of poor side effect management that’s similar to the transportation use case, it makes sense to really, for real, do integrative oncology and side effect management properly and proactively.
The four ruminations are:
1. The importance of the total cost of care and knowing what it is for financial and also health of members/patients/population reasons
2. Value-based drug or having a value mindset for purchasing almost anything may be cheaper than a cost containment mindset.
3. Some oncology centers are doing integrative oncology and side effect management for real and programmatically, and others are not. Meanwhile, where are the payers in all of this and how are they thinking about preventing avoidable dehydration readmissions? Question mark. While an employer, it does feel important to at least be aware that this is going on and ask questions about it of payers and providers etc.
4. I speculate there’s a fee-for-service business model for oncology centers to do side effect management, but they have to have a bead on their own data to know whether or not this is true.
So maybe my ruminations are sparking some ruminations of your own.
Also mentioned in this episode are Mark Lewis, MD; Celena Latham; Jun Mao, MD; Greg Green; Emily Kauff; Ethan Basch, MD; Nadine Jackson McCleary, MD, MPH, BSN; Glenn Sabin; Dan Mendelson; Cora Opsahl; Al Lewis; Shawn Gremminger; Nina Lathia, RPh, MSc, PhD; Barbara Wachsman; John Lee, MD; Erik Davis; Autumn Yongchu; Tom X. Lee, MD; Darrell Moon; and Buck Poropatich.
You can learn more at Blackstone and by connecting with Andreas on LinkedIn.
Andreas Mang is senior managing director, portfolio operations, and chief executive officer of Equity Healthcare, where he is involved in managing medical benefits spend across the Blackstone portfolio. Andreas brings 20 years of healthcare experience to Equity Healthcare, having held various roles in healthcare finance, operations, and strategy.
Prior to joining Blackstone, Andreas was the vice president responsible for national provider network operations at CareCentrix, a PE-backed, leading home health benefit-management company. At Blue Cross Blue Shield of Massachusetts, he held a variety of roles, including a leadership role identifying and implementing administrative cost savings opportunities throughout the organization and ultimately designing a new corporate business model. In addition, he held roles as the manager of strategic financial planning at Harvard Pilgrim Health Care and was a senior consultant with Deloitte Consulting’s Strategy and Operations group in Boston.
Andreas has a bachelor’s degree in healthcare management and policy from the University of New Hampshire and an MBA from the University of Rochester’s Simon School of Business Administration. He currently serves on the board of DECA Dental.
Stacey Richter uses her voice and thought leadership to provide insights for healthcare industry decision makers trying to do the right thing each week on Relentless Health Value. Each show features expert guests who break down the twists and tricks in the medical field to help improve outcomes and lower costs across the care continuum. Relentless Health Value is a top 100 podcast on iTunes in the medicine category and reaches tens of thousands of engaged listeners across the healthcare industry.
In addition to hosting Relentless Health Value, Stacey is co-president of QC-Health, a benefit corporation finding cost-effective ways to improve the health of Americans. She is also co-president of Aventria Health Group, a consultancy working with clients who endeavor to form collaborations with payers, providers, Pharma, employer organizations, or patient advocacy groups.
01:12 Andreas Mang on oncology medication side effect management.
03:12 Mark Lewis, MD’s Tweet.
03:39 Celena Latham’s response.
04:22 How integrative oncology can save money and what it looks like.
04:47 EP157 with Ethan Basch, MD.
06:20 Why PBMs saving money doesn’t necessarily mean savings for employers and payers.
07:36 EP435 with Dan Mendelson.
08:20 EP372 with Cora Opsahl.
08:40 EP331 with Al Lewis.
09:50 Stacey’s second rumination.
10:19 Why having a value mindset when purchasing is a thing.
10:42 Stacey’s third rumination.
12:03 EP370 with Erik Davis and Autumn Yongchu.
13:07 Why FFS does not pay or pay adequately for side effect management.
14:31 Stacey’s final rumination.
17:08 Summarizing Stacey’s four ruminations on this topic.
You can learn more at Blackstone and by connecting with Andreas on LinkedIn.
Andreas Mang of @blackstone and our host, Stacey Richter, discuss #financialtoxicity in #oncology #sideeffectmanagement on our #healthcarepodcast. #healthcare #podcast #financialhealth #primarycare #patientoutcomes #healthcareinnovation
Recent past interviews:
Click a guest’s name for their latest RHV episode!
Abby Burns and Stacey Richter, David Muhlestein, Luke Slindee, Dr John Lee, Brian Klepper, Elizabeth Mitchell, David Scheinker (Encore! EP363), Dan Mendelson, Dr Benjamin Schwartz, Justin Leader
538 episodes
Manage episode 425889353 series 2701020
Content provided by Stacey Richter. All podcast content including episodes, graphics, and podcast descriptions are uploaded and provided directly by Stacey Richter or their podcast platform partner. If you believe someone is using your copyrighted work without your permission, you can follow the process outlined here https://player.fm/legal.
This week, I’m gonna play an outtake, I guess it could be called, from the show with Andreas Mang from Blackstone that we wound up cutting for reasons of time and topic; but it’s been on my mind ever since. So, here’s this clip; and then I’m gonna invite you to partake in my ruminations because they hit the trifecta of employers and taxpayers and patients themselves getting taken for a ride from a cost perspective, while at the same time, patients are harmed. And the whole thing is so shortsighted.
Anyway, here’s the clip that started my downward spiral into … what’s the medical mental health term when you can’t stop rehashing something? Here’s the clip.
So, what is the number one … I gave it to you already, but I’ll just repeat it. Number one reason for readmissions, I think universally, if you looked at any health plan—and readmissions are bad, right? Bad quality and really expensive because something you went in for and came out, you’re back in, and it’s probably pretty bad. But the number one root cause of readmissions is dehydration associated with chemotherapy. Think how silly that is. Dehydration should not be the reason. So, you’re getting chemo, you’re feeling sick, you can’t keep down fluids, you’re vomiting, and so, you end up back in the hospital.
Well, guess what? There’s medications for that. Real simple, easy-to-take meds that’s the nausea so you can keep down fluids so you don’t get dehydrated. So, what have we done? In our world, on our platform—and health plans have tried to do this too, and they’ve done a reasonable job with their nurses and care managers—but like, in our world, we have an oncology trained nurse that is on your hip through your treatment as you go from Dr. Jones to Dr. Richter to Dr. Mang to doc, right? And none of us are talking to each other.
And so … but you have Nurse Sally on your hip talking to you whenever you want. At a minimum, they’re checking in with you, maybe it’s daily, during different bouts of treatment. “Hey, how you feeling today, Andreas?” I can’t keep down my … I’m nauseous. I’m not drinking anything. “Oh, let me call your doctor, let me get you a med, let’s get you that script that’s gonna suppress your nausea and be able to keep down fluids. You won’t end up back in the hospital.” Pretty simple solution, right?
So that was Andreas Mang, and go back and listen to the whole episode 419 about the whole way health benefits have become financialized in ways that CFOs and CEOs and boards of directors may want to be aware of—it’s not just people downstairs or in the warehouse who get cancer, after all—but also for all of the reasons which Andreas covers really well in that earlier episode. Andreas, by the way, is senior managing director at Blackstone and CEO of Equity Healthcare at Blackstone.
Let’s get this party started with a Tweet from Mark Lewis, MD. Mark Lewis is an oncologist, and he tweeted:
Dear insurance companies,
Anti-nausea medications signify one of the greatest advances in oncology.
Chemotherapy has to be effective, yes, but it has to be tolerable too. My patients risk getting sick every cycle. Please help me help them. It’s never been more important.
Then here’s what Celena Latham wrote in response to this Mark Lewis, MD, tweet. And if you go hunting around on Twitter or X or Facebook, you can find literally thousands of others saying the same basic thing.
Celena writes, “I fight with my insurance company all the time. They are happy to pay for my $10k-a-month chemo drug. But the $10-a-day nausea med is restricted. I am only allowed a 21-day supply at a time. The supply given is not enough.”
I was keeping all of this in the back of my mind when, in May, I was at the Memorial Sloan Kettering MSK Direct Day. And I heard a talk from Jun Mao, MD, that puts a lot of this in context. Dr. Mao presented a slide. Turns out, studies show, you can save $1 million per 100 cancer patients over three months by doing what’s called integrative oncology. And a big part of that, or a part of that, is managing treatment side effects like nausea and vomiting and thus keeping patients out of the ER for dehydration.
Thanks, by the way, very much to Greg Green and Emily Kauff for inviting me to that event. It was great.
Now, is this whole “hey, let’s manage oncology side effects” line of thinking some sort of breaking science? Let me refer you to a show I did with Ethan Basch, MD (EP157) in 2017. That was seven years ago. It is entitled “Major Improvements in Oncology Outcomes When Patients Self-Report Symptoms.”
In that interview, you can hear Dr. Basch talk about how he and his colleagues found that by doing things like managing side effects like nausea, patient survival time improved about five months. Those drugs that cost hundreds of thousands of dollars that are coming out, those immunology agents, many of them do not increase survival time this long.
So, not only are we talking about saving money here by managing side effects, but wait, there’s more. Survival time improves by an astounding amount, really, comparatively. We also had on the show in 2020 Nadine Jackson McCleary, MD, MPH, BSN, from Dana Farber and Harvard Medical School (EP254). She was talking about this. Oh, and also Glenn Sabin from FON Consulting in episode 233.
So, this is not news is the bottom line. And all of these kinds of facts and figures have been running through my mind while I’ve been ruminating over that outtake with Andreas Mang that I just played. Now let me get into the kind of the whys and the wherefores that I just really can’t stop rehashing.
First off, let’s just keep in mind, PBMs (pharmacy benefit managers) often have but one incentive, maybe but one job, depending on who you talk to and from where. And that one job is to lower drug costs, at least for themselves. Right now, some PBM is busy regaling their employer client about how much money they saved.
But let’s just say the quiet part out loud. In the oncology part of that spreadsheet, if the PBM restricts access to nausea meds, the employer will have lower PBM costs and higher medical costs. Let’s say the nausea med costs $5 a month, or even $1430 a month, which is the cost for a four-drug nausea and vomiting prophylaxis regimen, as per the NIH study I just read.
So, here’s me comparing that $5 to $1430 a month to the aforementioned $1 million saved on 100 cancer patients over three months stat that’s $3300 a month per patient. So, you know, PBM saves five bucks, a few hundred bucks, maybe even 1500 beans on the high end. And we spend $3300 on medical costs.
In this case, the downstream impact is also not gonna take years to accrue, so everybody wonders if they’re footing the bill for Medicare or somebody else who’s gonna receive that downstream cost savings. No, this is pretty immediate balloon squeezing, I would say. Right? Cancer patient has untreated nausea and vomiting. Cancer patient winds up in the ER.
Dan Mendelson talked about this in episode 435, by the way. He said—extremely crisply, I would add—plan sponsors gotta look at the total cost of care (ie, PBM, pharmacy spend, and medical spend together).
So that’s my first point to ponder, just the vital nature of aggregating PBM and medical data into a database of total costs. Which means that anybody trying to do population health can do their own math as opposed to relying on vendors to calculate their own “savings,” which anyone who has ever hired a point solution knows has the potential to not go well because it could enable somebody to “save” money in one place and cost a whole lot of money elsewhere.
Cora Opsahl also talks along these lines very compellingly in episode 372. She says if your data analyst can’t find savings opportunities—and, by the way, data analysts looking at the full dataset, such as the nausea example—but if they can’t find savings equivalent to their salary, then you have the wrong analyst, not a superior health plan.
Al Lewis talked about this also in great detail in episode 331. And furthermore, if we need one, I was also talking to Shawn Gremminger the other day from the National Alliance; and he said this exact same thing. Aggregate your data so you can see the total cost of care. Do your own math.
And look, I think everybody is saying this exact same thing because at least one goal is to spend less overall, not spend less on your way to spending more. Because that doesn’t count. This matters if you’re actually gonna succeed in cutting out waste and spend. But I might also scramble out on a limb and suggest that in probably a lot of instances, if you identify something that costs less in the short term but drives up the total cost of care—especially when that total cost of care is going up in a relatively short-term period—and if you know this and correct it by just spending a little bit more going in so that you spend less overall, you probably just fixed what is very likely a problem for patients in patient health. Feel free to agree or disagree on that point, but I bet I’m right.
That’s my first rumination. Just how this nausea from chemo is a great example of the why with you got to know the total cost of care.
My second rumination is just the whole thing with value-based drug purchasing or even medical purchasing, as opposed to cost-containment efforts that could spike costs elsewhere and/or cause a lot of presenteeism and absenteeism while the PBM vendor or maybe even the ASO (administrative services organization) or some provider organization gets a prize for controlling trend in the very short term, probably. Nina Lathia, RPh, MSc, PhD, talks about this in episode 426, and also Barbara Wachsman (EP430).
So, second point, having a value mindset when purchasing is a thing. Look, I’m just gonna state for the record that Blackstone knows how money works. And they have calculated, I would trust, that it is cheaper, at least for their populations, it is cheaper to manage chemo side effects than to not manage them. Or even worse, to restrict access to needed medications.
Which leads me to the third thing I’m thinking about as I consider how it can be that chemo side effects like nausea can possibly, in this day and age, go untreated or undertreated or undermanaged. I was talking to John Lee, MD (EP438) the other day; and he was talking about getting blood pressure readings from heart failure patients. (But trust me, I will bring this back to oncology patients left to their own devices in just one sec.) So, it turns out, the best way to get blood pressure readings from heart failure patients at home to make sure they don’t wind up in the ER and readmitted is have a nurse call them at home and ask them what their blood pressure is.
Works actually a lot better than any fancy stuff you might have been thinking of, but most provider organizations won’t do any dialing for blood pressure readings because they don’t get paid for it. And I’m pointing fingers all over the place and nowhere right now, but consider this blood pressure reading case study in the realm of managing oncology side effects like nausea.
For any given patient population, who is doing this side effect management? Does anyone know? Is anyone getting paid for it? And if no one is getting paid directly, then which hospitals are taking dollars they’re earning from buy and bill, which could be four to six times the cost of some of these oncology drugs (ie, a lot of money, lots of zeros)? Listen to episode 370 with Erik Davis and Autumn Yongchu for just how many zeros and how they’re doing it. But which oncology centers are taking these tens of thousands of dollars earned on the backs of buy and bill and using this money to run integrative oncology programs or manage side effects, like nausea?
A few do, don’t get me wrong; many do not. Or they don’t do nearly the stuff required as per the studies which demonstrate actual patient results. Like, you have to be collecting PROMs (patient-reported outcome measures) etc.
Tom X. Lee, MD, talks about this also in an upcoming show, this whole idea of having a value mindset and considering what good for patients looks like and then figuring out within current payment models how to make this happen so that patients get better care.
But also—and this can’t be understated—doctors and clinicians are happier and not morally fatigued by an obvious failure to, you know, not have patients spend the last three nights curled up on a towel under their toilet before heading to the ER to get hooked up to an IV. So that’s my point three rumination.
Fee for service (FFS) does not pay or pay adequately for stuff like making sure chemo patients, who, a lot of the time, will have side effects that can be costly. FFS does not pay to ensure they are proactively well managed. What FFS will pay for is waiting for the patients to fall off the cliff instead of preventing them from falling, as Darrell Moon often says. I guess this is the story of FFS, but this one, this whole nausea case study, pretty quickly has accruing costs financially and also from an employee emotional and physical impact standpoint.
So, back to that Andreas Mang quote, it seems like he and his team have concluded there could be a ton of variability in care. Providers may or may not have a value mindset and sufficient operational chops and may or may not choose to use dollars they earn off drugs or other services to do meaningful things that they may or may not get compensated for. This feels like something payers should be cognizant of because most employers don’t have resources Blackstone has to stand up their own nurse program when providers fail here.
And there also could be probably a pretty big equity consideration in the mix at the same time. But just point three, fee for service doesn’t pay for stuff like this. It’s gonna be up to a provider to choose to do it or not to do it. And all of that is a consideration for employers.
Here’s my last point I’m pondering, number four. And it also concerns what’s going on in or about oncology centers themselves. I thought of this while moderating a panel at the recent thINc Conference last month, and on this panel was Buck Poropatich from Lyft Healthcare. He said something fascinating. He said there’s two business cases for a health system to pay for transportation. And again, I’m gonna talk about transportation for a sec, but this is relevant to our oncology side effect management case study here.
So, two transportation case studies or two transportation business models: One is the value-based care arrangement business model, but let’s not talk about that one because it’s very obvious to most how dealing with social drivers of health is key when you are getting capitated payments to manage patient populations when you are, in fact, responsible for downstream costs of care; so, let’s just set aside the value-based care business model for transportation.
The business case I was fascinated by, though, is the fee-for-service business case for a hospital or provider organization to pay for transportation. It’s because no-shows are really expensive from a lost revenue perspective, and a lot of times the reason patients no-show is because they do not have transportation.
Or another use case is getting a patient discharged promptly to turn over a bed when the patient can’t get a ride home. If a health system is savvy enough to do the math, it might wind up being a profitable endeavor to pay for transportation for patients who need it. I started pondering this in the context of oncology center/provider organizations doing side effect management properly.
Is there an FFS/buy and bill “why” to stand up some of the care flows and do the outreaches and apps really well that are all necessary to do side effect management right? Is there a business case to do all of this in a fee-for-service environment?
Short answer: I don’t know, but I keep seeing studies showing that when side effects aren’t managed, courses of therapy are shortened (to the patient’s detriment we’re talking now in this use case) or doses are lowered or patients die prematurely. You would think that if someone at an oncology center was able to and did calculate the lost revenue from any or all of these downstream impacts of poor side effect management that’s similar to the transportation use case, it makes sense to really, for real, do integrative oncology and side effect management properly and proactively.
The four ruminations are:
1. The importance of the total cost of care and knowing what it is for financial and also health of members/patients/population reasons
2. Value-based drug or having a value mindset for purchasing almost anything may be cheaper than a cost containment mindset.
3. Some oncology centers are doing integrative oncology and side effect management for real and programmatically, and others are not. Meanwhile, where are the payers in all of this and how are they thinking about preventing avoidable dehydration readmissions? Question mark. While an employer, it does feel important to at least be aware that this is going on and ask questions about it of payers and providers etc.
4. I speculate there’s a fee-for-service business model for oncology centers to do side effect management, but they have to have a bead on their own data to know whether or not this is true.
So maybe my ruminations are sparking some ruminations of your own.
Also mentioned in this episode are Mark Lewis, MD; Celena Latham; Jun Mao, MD; Greg Green; Emily Kauff; Ethan Basch, MD; Nadine Jackson McCleary, MD, MPH, BSN; Glenn Sabin; Dan Mendelson; Cora Opsahl; Al Lewis; Shawn Gremminger; Nina Lathia, RPh, MSc, PhD; Barbara Wachsman; John Lee, MD; Erik Davis; Autumn Yongchu; Tom X. Lee, MD; Darrell Moon; and Buck Poropatich.
You can learn more at Blackstone and by connecting with Andreas on LinkedIn.
Andreas Mang is senior managing director, portfolio operations, and chief executive officer of Equity Healthcare, where he is involved in managing medical benefits spend across the Blackstone portfolio. Andreas brings 20 years of healthcare experience to Equity Healthcare, having held various roles in healthcare finance, operations, and strategy.
Prior to joining Blackstone, Andreas was the vice president responsible for national provider network operations at CareCentrix, a PE-backed, leading home health benefit-management company. At Blue Cross Blue Shield of Massachusetts, he held a variety of roles, including a leadership role identifying and implementing administrative cost savings opportunities throughout the organization and ultimately designing a new corporate business model. In addition, he held roles as the manager of strategic financial planning at Harvard Pilgrim Health Care and was a senior consultant with Deloitte Consulting’s Strategy and Operations group in Boston.
Andreas has a bachelor’s degree in healthcare management and policy from the University of New Hampshire and an MBA from the University of Rochester’s Simon School of Business Administration. He currently serves on the board of DECA Dental.
Stacey Richter uses her voice and thought leadership to provide insights for healthcare industry decision makers trying to do the right thing each week on Relentless Health Value. Each show features expert guests who break down the twists and tricks in the medical field to help improve outcomes and lower costs across the care continuum. Relentless Health Value is a top 100 podcast on iTunes in the medicine category and reaches tens of thousands of engaged listeners across the healthcare industry.
In addition to hosting Relentless Health Value, Stacey is co-president of QC-Health, a benefit corporation finding cost-effective ways to improve the health of Americans. She is also co-president of Aventria Health Group, a consultancy working with clients who endeavor to form collaborations with payers, providers, Pharma, employer organizations, or patient advocacy groups.
01:12 Andreas Mang on oncology medication side effect management.
03:12 Mark Lewis, MD’s Tweet.
03:39 Celena Latham’s response.
04:22 How integrative oncology can save money and what it looks like.
04:47 EP157 with Ethan Basch, MD.
06:20 Why PBMs saving money doesn’t necessarily mean savings for employers and payers.
07:36 EP435 with Dan Mendelson.
08:20 EP372 with Cora Opsahl.
08:40 EP331 with Al Lewis.
09:50 Stacey’s second rumination.
10:19 Why having a value mindset when purchasing is a thing.
10:42 Stacey’s third rumination.
12:03 EP370 with Erik Davis and Autumn Yongchu.
13:07 Why FFS does not pay or pay adequately for side effect management.
14:31 Stacey’s final rumination.
17:08 Summarizing Stacey’s four ruminations on this topic.
You can learn more at Blackstone and by connecting with Andreas on LinkedIn.
Andreas Mang of @blackstone and our host, Stacey Richter, discuss #financialtoxicity in #oncology #sideeffectmanagement on our #healthcarepodcast. #healthcare #podcast #financialhealth #primarycare #patientoutcomes #healthcareinnovation
Recent past interviews:
Click a guest’s name for their latest RHV episode!
Abby Burns and Stacey Richter, David Muhlestein, Luke Slindee, Dr John Lee, Brian Klepper, Elizabeth Mitchell, David Scheinker (Encore! EP363), Dan Mendelson, Dr Benjamin Schwartz, Justin Leader
538 episodes
همه قسمت ها
×Welcome to Player FM!
Player FM is scanning the web for high-quality podcasts for you to enjoy right now. It's the best podcast app and works on Android, iPhone, and the web. Signup to sync subscriptions across devices.
Similar to Relentless Health Value™
PT Inquest is an online journal club. Hosted by Jason Tuori, Megan Graham, and Chris Juneau, the show looks at an article every week and discusses how it applies to current physical therapy practice.
…
continue reading
A daily dose of irreverent, offbeat, and informative takes on business & tech news. Hosted by Jon Weigell, Juliet Bennett Rylah, Mark Dent, Ben Berkley, Sara Friedman and Rob Litterst from The Hustle.
…
continue reading
Bloomberg Daybreak delivers today's top stories, with context, in just 15 minutes. Get informed from Bloomberg's 2,700 journalists and analysts in 120 countries.
…
continue reading
The economy and the markets are "under surveillance" as we cover the latest in finance, economics and investment. Listen to Jonathan Ferro, Lisa Abramowicz and Annmarie Hordern for the top interviews from Bloomberg Surveillance Television. And join Tom Keene and Paul Sweeney for the best conversations from Bloomberg Surveillance Radio. Watch Surveillance TV LIVE each mornings: http://bit.ly/3P7nstQ. Watch Surveillance Radio LIVE weekday mornings: http://bit.ly/3vTiACF.
…
continue reading
The American healthcare system is one of the most innovative in the world. But it’s also riddled with complex challenges, such as access to affordable medications, inefficiency and administrative burdens, and communication barriers between providers. There’s clearly a better way—and at Surescripts, we have a unique sightline into what that may be. In this series, host Melanie Marcus, Chief Marketing Officer of Surescripts, sits down with today’s most inspiring and innovative leaders in healt ...
…
continue reading
Tempers fly as the newsmakers of the week face-off in this award-winning show. Anchored by Sanket Upadhyay, this weekly program has politicians battlling wits with a live audience.
…
continue reading
Join Larry Mantle weekdays for lively and in-depth discussions of Los Angeles and Southern California news, politics, science, entertainment, the arts and more. More AirTalk at www.kpcc.org.
…
continue reading
Brilliant solutions to the world’s problems. We meet people with ideas to make the world a better place and investigate whether they work.
…
continue reading
A handpicked article read aloud from the latest issue of The Economist. Published weekdays from Monday to Thursday. If you’re already a subscriber to The Economist, you’ll have full access to all our shows as part of your subscription. For more information about Economist Podcasts+, including how to get access, please visit our FAQs page here https://myaccount.economist.com/s/article/What-is-Economist-Podcasts.
…
continue reading
Introducing the BODi® Partner Podcast, the official podcast channel devoted exclusively to BODi Partners. From archives of the BODi Wake-Up Call, I Am BODi stories, and What I Know Now success tips from seasoned Partners, this podcast is your one-stop source for personal development, business training and peer-to-peer inspiration. Ready to explode your business? Tune in regularly to our official podcast and join the ranks of those transforming their lives and the lives of others!
…
continue reading
Player FM - Podcast App
Go offline with the Player FM app!
Go offline with the Player FM app!



{kind=link}