PT Inquest is an online journal club. Hosted by Jason Tuori, Megan Graham, and Chris Juneau, the show looks at an article every week and discusses how it applies to current physical therapy practice.
…
continue reading
Content provided by PulmPEEPs. All podcast content including episodes, graphics, and podcast descriptions are uploaded and provided directly by PulmPEEPs or their podcast platform partner. If you believe someone is using your copyrighted work without your permission, you can follow the process outlined here https://player.fm/legal.
Similar to PulmPEEPs
The Art of Charm is where self-motivated people, just like you, come to learn from the company’s coaches about to how to master human dynamics, relationships, and becoming your best self with the help of Johnny and AJ, the company’s founders. Johnny and AJ bring their 11 years of coaching experience from their famous Bootcamps, where they host clients in Los Angeles from all over the world and they share their stories, best practices and themselves on this weekly podcast. Not only does The A ...
…
continue reading
Although the world is becoming mostly sedentary, our bodies still require a wide variety of daily movements in order to work well. Many of us struggle to get regular exercise, but even that can fall short of nourishing the body from head to toe. How can we move more—a lot more—when we have sore, stiff parts and overly busy lifestyles? Join Katy Bowman M.S., biomechanist, author, and movement educator as she combines big-picture lessons on biomechanics, kinesiology, physiology, and natural hu ...
…
continue reading
Five-time winner of Best Education Podcast in the Podcast Awards. Grammar Girl provides short, friendly tips to improve your writing and feed your love of the English language. Whether English is your first language or your second language, these grammar, punctuation, style, and business tips will make you a better and more successful writer. Grammar Girl is a Quick and Dirty Tips podcast.
…
continue reading
We are often distracted in life and never really dive deep into the real foundation of self improvement, goal achieving, and wellbeing. - Join our team of experts every week as we discuss the real facets of manhood. Topics like: How to develop more self esteem, self love, deeper relationships. How to improve our wellbeing, mental toughness, resilience, and productivity. How to develop critical skills, become better leaders, expand our careers/business, create financial security and contribut ...
…
continue reading
Introducing the BODi® Partner Podcast, the official podcast channel devoted exclusively to BODi Partners. From archives of the BODi Wake-Up Call, I Am BODi stories, and What I Know Now success tips from seasoned Partners, this podcast is your one-stop source for personal development, business training and peer-to-peer inspiration. Ready to explode your business? Tune in regularly to our official podcast and join the ranks of those transforming their lives and the lives of others!
…
continue reading
Learn the Spartan mindset. Founder & CEO of Spartan Race and NY Times best-selling author, travels the globe seeking and answers authors, academics, athletes, adventurers, entrepreneurs, CEOs and thought leaders. It will shift your thinking, make you laugh and and give you the tools you need. He’s on a mission to find the secrets to success in all aspects of life. Not only does Joe interview epic people, he has brought together an amazing panel to break down and analyze every aspect of these ...
…
continue reading
The Voice of ASWJ Australia. Listen to & Download Our Latest Programs. Topics: Aqeedah (Creed), Tafsir Qur'an, Islamic Fiqh, History, Youth & Community programs, Medical & Health programs and much much more. Podcasts are in Arabic & English.
…
continue reading
Everyone has a dream. But sometimes there’s a gap between where we are and where we want to be. True, there are some people who can bridge that gap easily, on their own, but all of us need a little help at some point. A little boost. An accountability partner. A Snooze Squad. In each episode, the Snooze Squad will strategize an action plan for people to face their fears. Guests will transform their own perception of their potential and walk away a few inches closer to who they want to become ...
…
continue reading
Seeking a healthier emotional life? It’s time to bring a trained psychologist and mental health expert along for the ride. Dr. Monica Johnson explains the why behind complex emotions, helps you form better relationships, and guides you down the path of self-understanding.
…
continue reading
Player FM - Podcast App
Go offline with the Player FM app!
Go offline with the Player FM app!

))
76. Fellows’ Case Files: University of Rochester
Manage episode 429448149 series 3299598
Content provided by PulmPEEPs. All podcast content including episodes, graphics, and podcast descriptions are uploaded and provided directly by PulmPEEPs or their podcast platform partner. If you believe someone is using your copyrighted work without your permission, you can follow the process outlined here https://player.fm/legal.
Today we’re back with another stop on our Fellows’ Case Files journey and making our way to the University of Rochester. Tune in to hear about this fascinating case and learn some key teaching points along the way.
Meet Our Guests
Dr. Shiv Patel completed his IM residency and a Chief year at the California Pacific Medical Center- Van Ness Campus and is currently a second-year PCCM fellow at the University of Rochester.
Dr. Mary Anne Morgan is an Associate Professor of Medicine and the Fellowship Program Director for the PCCM Fellowship at the University of Rochester. Her clinical interests range from the care of critically ill patients in the ICU to the diagnosis and management of rare lung disease in her role as Director of the University of Rochester LAM Clinic. She loves unwrapping clinical reasoning with trainees, exploring issues around communication and teamwork in the ICU, and is excited about curriculum revitalization in the growing URMC PCCM fellowship program.
Case Presentation
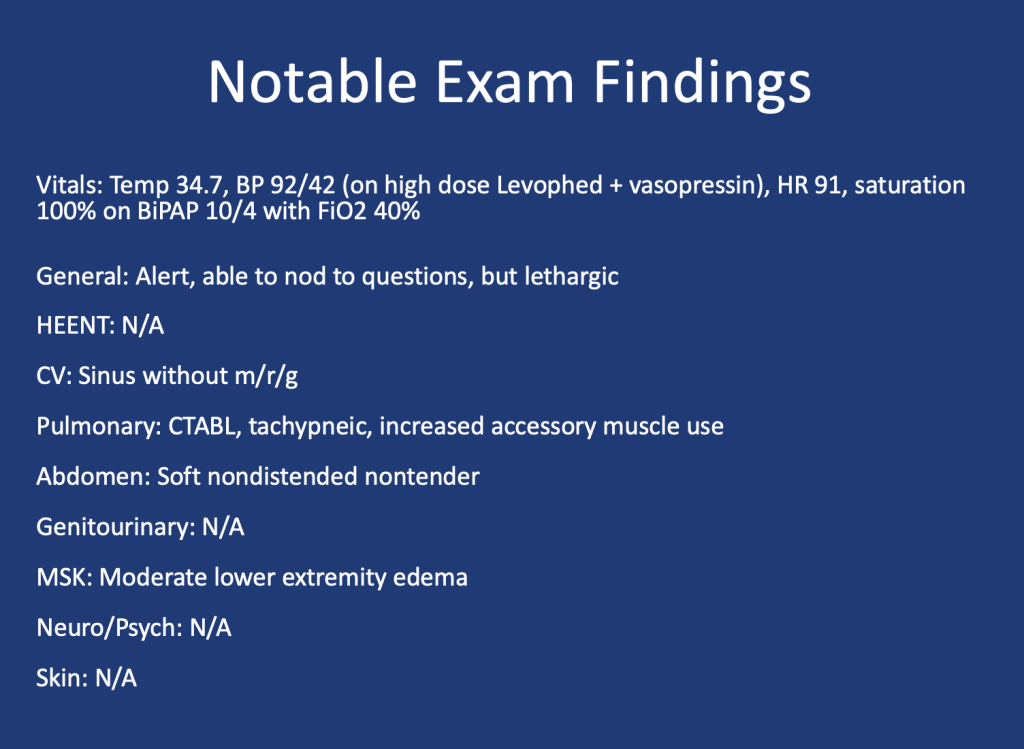
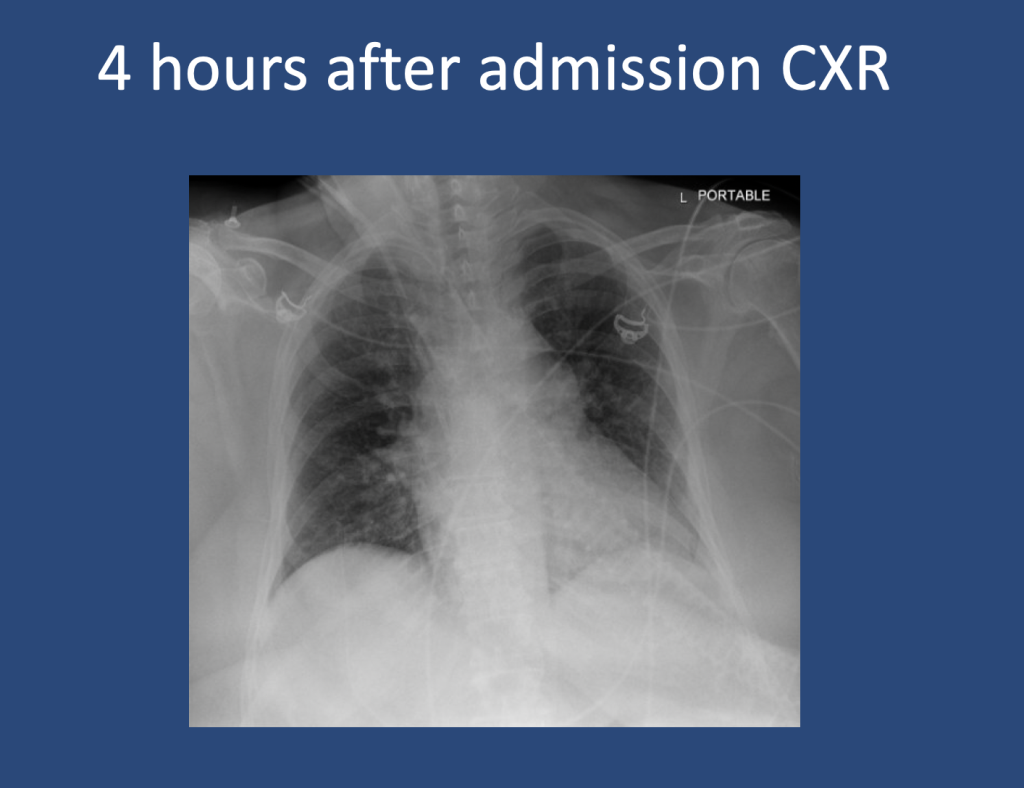
A 75 y.o. female with a history of Hypertension, Hyperlipidemia, and Type 2 Diabetes presented for evaluation of hypoglycemia and generalized fatigue. She had felt poorly for about a week with symptoms of back pain, generalized weakness, and dyspnea, all of which acutely worsened on the day of presentation.
She was found to be hypoglycemic with a blood glucose level in the to 40’s. Initial vital signs included a heart rate of 56, blood pressure of 70/40, respiratory rate of 30, and temperature of 28.5 degrees Celsius.
Key Learning Points
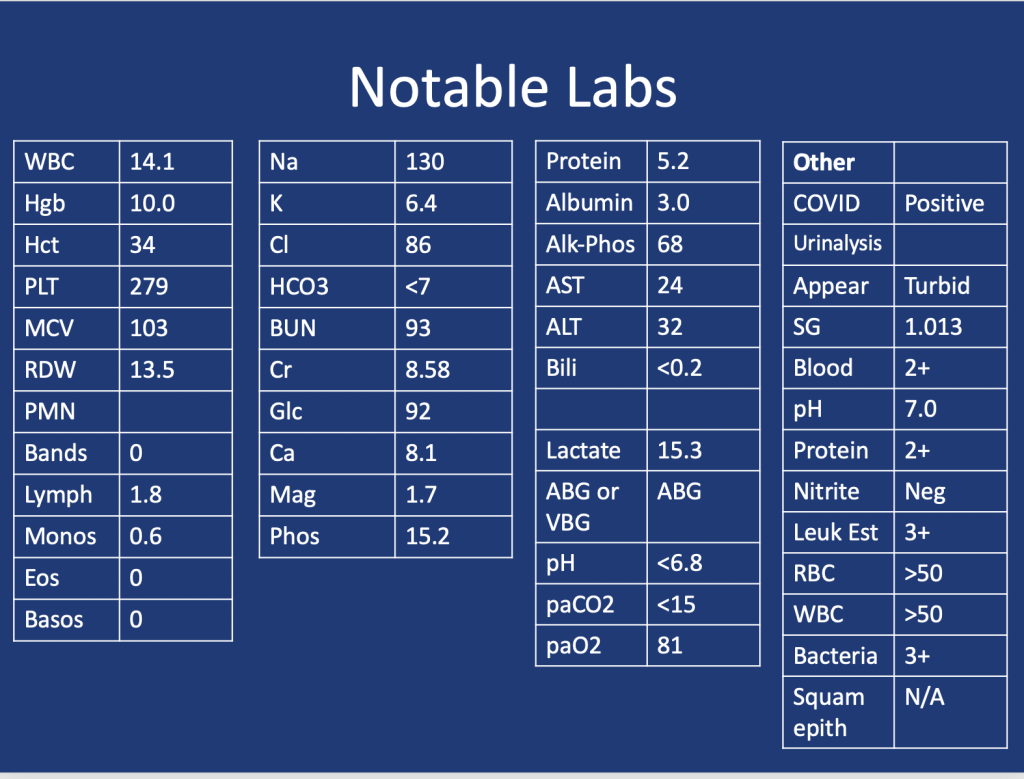
Lactic Acidosis: Type A, Type B and Type D
Type A: Typically secondary to conditions that impair oxygen delivery (respiratory failure, PE) to tissues or decrease tissue perfusion (severe anemia, shock). Patients typically present with hypotension, tachycardia, tachypnea, altered mental status, and signs of organ dysfunction.
Type B: Typically secondary to conditions that directly affect cellular metabolism or lactate clearance and characterized by the presence of hyperlactatemia without evidence of tissue hypoperfusion or hypoxia. Conditions associated include liver dysfunction (e.g., liver failure, cirrhosis), malignancies (especially hematological malignancies), medications/toxins (e.g., metformin, cyanide poisoning), inborn errors of metabolism, and mitochondrial disorders.
Type D: Less common presentation and can be seen in patients with short gut syndrome.
References
1.Blough B, Moreland A, Mora A Jr. Metformin-induced lactic acidosis with emphasis on the anion gap. Proc (Bayl Univ Med Cent). 2015 Jan;28(1):31-3. doi: 10.1080/08998280.2015.11929178. PMID: 25552792; PMCID: PMC4264704.
2.Callelo et al. Extracorporeal Treatment for Metformin Poisoning: Systematic Review and Recommendations From the Extracorporeal Treatments in Poisoning Workgroup. DOI: 10.1097/CCM.0000000000001002
3.Friesecke, S., Abel, P., Roser, M. et al. Outcome of severe lactic acidosis associated with metformin accumulation. Crit Care 14, R226 (2010). https://doi.org/10.1186/cc9376
4.Madias NE. Lactic acidosis. Kidney Int. 1986 Mar;29(3):752-74. doi: 10.1038/ki.1986.62. PMID: 3702227.
5. Stiller RH, Luks AM, Çoruh B. All That Raises Lactate Is Not Sepsis. ATS Sch. 2023 Jun 12;4(3):385-386. doi: 10.34197/ats-scholar.2023-0032OT.
81 episodes
Manage episode 429448149 series 3299598
Content provided by PulmPEEPs. All podcast content including episodes, graphics, and podcast descriptions are uploaded and provided directly by PulmPEEPs or their podcast platform partner. If you believe someone is using your copyrighted work without your permission, you can follow the process outlined here https://player.fm/legal.
Today we’re back with another stop on our Fellows’ Case Files journey and making our way to the University of Rochester. Tune in to hear about this fascinating case and learn some key teaching points along the way.
Meet Our Guests
Dr. Shiv Patel completed his IM residency and a Chief year at the California Pacific Medical Center- Van Ness Campus and is currently a second-year PCCM fellow at the University of Rochester.
Dr. Mary Anne Morgan is an Associate Professor of Medicine and the Fellowship Program Director for the PCCM Fellowship at the University of Rochester. Her clinical interests range from the care of critically ill patients in the ICU to the diagnosis and management of rare lung disease in her role as Director of the University of Rochester LAM Clinic. She loves unwrapping clinical reasoning with trainees, exploring issues around communication and teamwork in the ICU, and is excited about curriculum revitalization in the growing URMC PCCM fellowship program.
Case Presentation
A 75 y.o. female with a history of Hypertension, Hyperlipidemia, and Type 2 Diabetes presented for evaluation of hypoglycemia and generalized fatigue. She had felt poorly for about a week with symptoms of back pain, generalized weakness, and dyspnea, all of which acutely worsened on the day of presentation.
She was found to be hypoglycemic with a blood glucose level in the to 40’s. Initial vital signs included a heart rate of 56, blood pressure of 70/40, respiratory rate of 30, and temperature of 28.5 degrees Celsius.
Key Learning Points
Lactic Acidosis: Type A, Type B and Type D
Type A: Typically secondary to conditions that impair oxygen delivery (respiratory failure, PE) to tissues or decrease tissue perfusion (severe anemia, shock). Patients typically present with hypotension, tachycardia, tachypnea, altered mental status, and signs of organ dysfunction.
Type B: Typically secondary to conditions that directly affect cellular metabolism or lactate clearance and characterized by the presence of hyperlactatemia without evidence of tissue hypoperfusion or hypoxia. Conditions associated include liver dysfunction (e.g., liver failure, cirrhosis), malignancies (especially hematological malignancies), medications/toxins (e.g., metformin, cyanide poisoning), inborn errors of metabolism, and mitochondrial disorders.
Type D: Less common presentation and can be seen in patients with short gut syndrome.
References
1.Blough B, Moreland A, Mora A Jr. Metformin-induced lactic acidosis with emphasis on the anion gap. Proc (Bayl Univ Med Cent). 2015 Jan;28(1):31-3. doi: 10.1080/08998280.2015.11929178. PMID: 25552792; PMCID: PMC4264704.
2.Callelo et al. Extracorporeal Treatment for Metformin Poisoning: Systematic Review and Recommendations From the Extracorporeal Treatments in Poisoning Workgroup. DOI: 10.1097/CCM.0000000000001002
3.Friesecke, S., Abel, P., Roser, M. et al. Outcome of severe lactic acidosis associated with metformin accumulation. Crit Care 14, R226 (2010). https://doi.org/10.1186/cc9376
4.Madias NE. Lactic acidosis. Kidney Int. 1986 Mar;29(3):752-74. doi: 10.1038/ki.1986.62. PMID: 3702227.
5. Stiller RH, Luks AM, Çoruh B. All That Raises Lactate Is Not Sepsis. ATS Sch. 2023 Jun 12;4(3):385-386. doi: 10.34197/ats-scholar.2023-0032OT.
81 episodes
All episodes
×Welcome to Player FM!
Player FM is scanning the web for high-quality podcasts for you to enjoy right now. It's the best podcast app and works on Android, iPhone, and the web. Signup to sync subscriptions across devices.
Similar to PulmPEEPs
PT Inquest is an online journal club. Hosted by Jason Tuori, Megan Graham, and Chris Juneau, the show looks at an article every week and discusses how it applies to current physical therapy practice.
…
continue reading
The Art of Charm is where self-motivated people, just like you, come to learn from the company’s coaches about to how to master human dynamics, relationships, and becoming your best self with the help of Johnny and AJ, the company’s founders. Johnny and AJ bring their 11 years of coaching experience from their famous Bootcamps, where they host clients in Los Angeles from all over the world and they share their stories, best practices and themselves on this weekly podcast. Not only does The A ...
…
continue reading
Although the world is becoming mostly sedentary, our bodies still require a wide variety of daily movements in order to work well. Many of us struggle to get regular exercise, but even that can fall short of nourishing the body from head to toe. How can we move more—a lot more—when we have sore, stiff parts and overly busy lifestyles? Join Katy Bowman M.S., biomechanist, author, and movement educator as she combines big-picture lessons on biomechanics, kinesiology, physiology, and natural hu ...
…
continue reading
Five-time winner of Best Education Podcast in the Podcast Awards. Grammar Girl provides short, friendly tips to improve your writing and feed your love of the English language. Whether English is your first language or your second language, these grammar, punctuation, style, and business tips will make you a better and more successful writer. Grammar Girl is a Quick and Dirty Tips podcast.
…
continue reading
We are often distracted in life and never really dive deep into the real foundation of self improvement, goal achieving, and wellbeing. - Join our team of experts every week as we discuss the real facets of manhood. Topics like: How to develop more self esteem, self love, deeper relationships. How to improve our wellbeing, mental toughness, resilience, and productivity. How to develop critical skills, become better leaders, expand our careers/business, create financial security and contribut ...
…
continue reading
Introducing the BODi® Partner Podcast, the official podcast channel devoted exclusively to BODi Partners. From archives of the BODi Wake-Up Call, I Am BODi stories, and What I Know Now success tips from seasoned Partners, this podcast is your one-stop source for personal development, business training and peer-to-peer inspiration. Ready to explode your business? Tune in regularly to our official podcast and join the ranks of those transforming their lives and the lives of others!
…
continue reading
Learn the Spartan mindset. Founder & CEO of Spartan Race and NY Times best-selling author, travels the globe seeking and answers authors, academics, athletes, adventurers, entrepreneurs, CEOs and thought leaders. It will shift your thinking, make you laugh and and give you the tools you need. He’s on a mission to find the secrets to success in all aspects of life. Not only does Joe interview epic people, he has brought together an amazing panel to break down and analyze every aspect of these ...
…
continue reading
The Voice of ASWJ Australia. Listen to & Download Our Latest Programs. Topics: Aqeedah (Creed), Tafsir Qur'an, Islamic Fiqh, History, Youth & Community programs, Medical & Health programs and much much more. Podcasts are in Arabic & English.
…
continue reading
Everyone has a dream. But sometimes there’s a gap between where we are and where we want to be. True, there are some people who can bridge that gap easily, on their own, but all of us need a little help at some point. A little boost. An accountability partner. A Snooze Squad. In each episode, the Snooze Squad will strategize an action plan for people to face their fears. Guests will transform their own perception of their potential and walk away a few inches closer to who they want to become ...
…
continue reading
Seeking a healthier emotional life? It’s time to bring a trained psychologist and mental health expert along for the ride. Dr. Monica Johnson explains the why behind complex emotions, helps you form better relationships, and guides you down the path of self-understanding.
…
continue reading
Player FM - Podcast App
Go offline with the Player FM app!
Go offline with the Player FM app!



